
Alternative Treatment Plans: Implant-Supported Mandibular Dentures
Keith D. Rossein
Data from the 1988-1991 Oral Health Survey by the National Institute of Dental Research indicated that approximately 28 million Americans were completely edentulous.1 By the year 2020, 53 million Americans will be 65 years of age or older.2 Aging populations result in increased mandibular edentulism. Without stimulation from teeth or implants and with constant rubbing and pressure from the hard denture base, vertical bone loss in the edentulous mandible averages 1 mm to 3 mm per year.3
With the average American living longer, having more disposable income, and seeking better health care, implants have become a realistic alternative for the partially or completely edentulous individual.
Implant-retained or implant-supported removable dentures often offer significant advantages for many patients over fixed bridgework. Usually, the procedure requires fewer implants and component parts; the buccal flanges of the overdenture can provide excellent soft tissue support of the cheeks and lips; treatment time is reduced in comparison; overall cost to the patient is considerably lower; and for elderly, frail, or disabled patients, oral hygiene and home care are simpler and easier to accomplish.
There are a number of proven alternative implant treatment plans that can provide stabilization, retention, or support of the patient’s denture. Attachments, composed of two or more parts, are used to gain retention. One part is incorporated into the denture and the other part connects to the implant.
Attachments are categorized as either precision (machined from distinctive alloy) or semi-precision (cast from wax or plastic patterns). Attachments may be further subdivided into radicular studs or bar types. The bar attachment rigidly connects two or more implants together over an edentulous space. The stud attachment connects directly to the free-standing implants, usually by screws. Attach-ments for implant-supported dentures should be resilient to allow maximum contact of the denture with the oral mucosa during chewing.3
The ball attachment, screwed into two or three freestanding implants, is commonly used. The ball interlocks into a corresponding female attachment with an O-ring retrofitted to the denture base. It is both implant- and mucosa-supported. In many cases, a denture is retrofitted over a round cast bar that is firmly attached to two implants by screwing it into position. Hader or Dolder bars accomplish the same effect. A metal clip embedded into the denture is retained by the ovoid section of the bar (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5).
There is a good percentage of individuals who have been neglected as candidates for implant overdentures because their ridges are too thin, the vertical height of available bone has been severely compromised, and/or the existing denture-base height necessary to retrofit the den-ture is inadequate. Now an alternative technique using narrow-body implants have solved these problems and, by comparison, offers great advantages to both the patient and dentist. The length of treatment time is significantly reduced because the surgical portion foregoes the traditional two-stage surgery. The narrow-body implants are placed without reflecting a flap and are immediately loaded. Because there are little to no laboratory fees and the implants/components are less costly, the procedure is more affordable to a greater number of patients. Problems with limited space have been addressed by implant companies by offering implants with diameters such as 1.8 mm, 2.2 mm, 2.4 mm, 2.5 mm, and 2.8 mm.
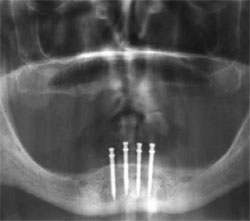
There are eight or nine manufacturers of narrow-body implants suitable for the overdenture technique. One system, Atlas™ (Dentatus USA, New York, NY), stands alone in that it requires no O-rings, copings, or housings, but instead uses a nonporous silicone reline material that attaches mechanically to the patient’s denture and grips the oversized heads of the implants to provide retention, stabilization, and cushioning on the patient’s ridge (Figure 6). It is recommended that four Atlas implants be placed anterior to the mental foramen (Figure 7 and Figure 8).
This design has solved many of the problems associated with other systems that use copings and O-rings. Copings are fixed housings that can cause undue pressure and lateral forces on the implants during mastication and each time the dentures are removed or inserted, especially if the implants are not parallel to each other. The resulting micromovement often leads to loosening and possibly the loss of an implant. Because of the resiliency of the TufLink™ (Dentatus USA) silicone reline material and the lack of copings or O-rings associated with this technique, parallel discrepancies are insignificant. Most other narrow-bodied systems have small retentive heads. The Atlas implant head is much larger than the implant body, creating better retention. The entire procedure of placing the Atlas implants and relining with the TufLink silicone will take about 1 hour.
ACKNOWLEDGMENTS
The author wishes to thank Dr. James Pavlatos for providing Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Dr. Andrew Kelly for Figure 6, and Dr. Ziv Mazor for Figure 7 and Figure 8.
REFERENCES
1. Marcus SE, Drury TF, Brown LJ, et al. Tooth retention and tooth loss in the permanent dentition of adults: United States, 1988-1991. J Dent Res. 1996;75(Spec No):684-695.
2. NHTSA 2020 Report. 1997. Available at: www.nhtsa.dot.gov. Accessed May 12, 2006.
3. Pavlatos J. Mandibular implant-supported overdentures. Implant News & Views. 2001;3(3):6-8.
 |
 |
||||
| Figure 1 Ball attachment abutments placed directly into the implants (Innova Corporation, Toronto, Ontario, Canada). | Figure 2 Simple bar attached to two implants. The overdenture is retained with an anterior metal clip. | ||||
 |
 |
||||
| Figure 3 Intraoral placement of Zaag low-profile bar (Zest Anchors, Escondido, CA). | Figure 4 Zaag implant anchors screwed into implants (Zest Anchors). | ||||
 |
 |
||||
| Figure 5 Mandibular overdenture with distal ERA® nylon male connectors and two metal clips (Sterngold Dental, LLC, Attleboro, MA). | Figure 6 Denture base with TufLink silicone reline that grips the implant heads for retention (Dentatus USA). | ||||
 |
 |
||||
| Figure 7 Four Atlas implants placed anterior to the mental foramen. Notice the oversized head (Dentatus USA, New York, NY). | Figure 8 Radiograph of Atlas implants placed without flap surgery. | ||||
|
|||||


