
Education in the Round: Multidimensional Imaging in Dentistry
Allan G. Farman, BDS, PhD, MBA, DSc; Claudio M. Levato, DDS; William C. Scarfe, BDS, MS; and James Mah, DDS
“A Primer on Cone Beam CT” was published in the January 2007 issue of Inside Dentistry and a follow-up article, “3-D X-Ray: An Update” appeared in June 2007. We noted in those articles that the application of cone beam computed tomography (CBCT) has taken dentistry by storm. The purpose of this sequel is to provide an update on existing and emerging systems and allied technologies based on continuing education demonstrations and exhibits at the 148th American Dental Association (ADA) Annual Session held in San Francisco, September 26-30, 2007. In particular, we will review the imaging software and service add-ons that were demonstrated to work with CBCT image data sets.
In the fall of 2006, the primary author was contacted by Richard Schuch, ADA senior manager for program development, with an invitation to participate in a new form of continuing education, “Education in the Round” (Figure 1). The audience would be seated around a central stage area where live patient care would be demonstrated and shown in real time on a circular array of eight large plasma screens. The topic would be CBCT, with as many different units demonstrated as practical for the space and time constraints.
Immediately, all of the reasons that this would be difficult to achieve were raised. There would be need for substantial radiation barriers that were entirely transparent so that the audience could see what was happening, not just on the screens but directly. There would be need for clearance from the California State Regulators for the use of ionizing radiation, permissions from the Moscone Congress Center and the California Board of Dentistry, and HIPAA releases for patients with a defined diagnostic referral need. Further, there were structural considerations for the placement of four systems and their supports in a limited area, in addition to their calibration and removal, in a relatively short turn-around time after the event.
While such issues seemed almost insolvable, Mr. Schuch was able to deliver all of the necessary permits and facilities to make this series happen. Thomas Schiff, DMD, former chair of oral and maxillofacial radiology at the University of the Pacific, San Francisco, successfully recruited the eight patients needed to demonstrate four CBCT systems in two separate sessions. Dale Miles, DDS, MS, and James Mah, DDS, were the other two presenting clinicians. The four CBCT systems included in the 2007 demonstration were the Next Generation i-CAT® (Imaging Sciences International, Hatfield, PA), the NewTom VG (Dent-X, Elmsford, NY), the ILUMA™ Ultra Cone Beam CT (Imtec Corporation, Ardmore, OK), and the Galileos (Sirona Dental Systems LLC, Charlotte, NC).
This program was not intended as a “shoot out” comparison between systems, but rather to introduce the concept of CBCT, to demonstrate the convenience of workflow, and to examine the export of digital imaging and communication in medicine (DICOM) datasets from the representative systems to third-party software and for add-on services that are in the process of revolutionizing the way that dental practice is performed. This was an ADA-CERP approved educational activity rather than a commercial for any particular products.
The first two sessions demonstrated image production, immediate processing, export to third-party software, and secure dataset transmission. A third session demonstrated add-on services, including model and positioning stent preparation from CBCT datasets. It also provided a live demonstration of 3-dimensional (3-D) photograph production by 3dMD (Atlanta, GA) with the fusion of obtained photographic data to CBCT volumetric reconstructions.
CBCT SYSTEMS SHOWN AT THE ADA 2007
In addition to the four systems demonstrated in the “Education in the Round” session, the following Food and Drug Administration (FDA)-approved systems were exhibited at ADA 2007: the NewTom QR DVT 3G (Dent-X), the 3D Accuitomo (J. Morita USA, Inc, Irvine, CA), the Planmeca Promax 3D (Planmeca, Helsinki, Finland), Picasso Trio (E-Woo Technology USA, Houston, TX), and PreXion 3D (TeraRecon, Inc, San Mateo, CA).
Soredex (Helsinki, Finland) exhibited the Scanora 3D as a work in process as the unit was still awaiting FDA approval. Belmont (Somerset, NJ) exhibited the Quolis® Alphard 3030, which was also awaiting FDA approval.
Hitachi did not exhibit its FDA-approved CB MercuRay and there is apparently no immediate plan to launch the CB Throne, a smaller CBCT unit sold in Japan, to the US market. Likewise, J. Morita did not exhibit its Veraviewepocs® 3D at ADA as it is still awaiting FDA approval, and MyRay (Imolo, Italy) did not exhibit its SkyView CBCT concept.
Additional CBCT units from Instrumentarium Dental Inc (Milwaukee, WI) (full volume) and Kodak (Atlanta, GA) (limited volume) are expected in the not-too-distant future, as prototypes of the former are on trial in Europe and sale of the latter has already been announced in France with a word-of-mouth price of 85,000 EUR (~$120,000 USD).
Consumer choice in the United States is growing and will expand. The lowest “special” ADA Annual Session price was around $127,000 for a “no thrills,” complete, limited-volume CBCT system, with most CBCT units still in the $150,000 to $250,000 price range. The cost of setting up a room for housing the system should also be factored in; leaded acrylic panels can easily be more than $10,000. Additionally, one should include approximately $10,000 per annum for extended warranty support and software updates.
YOU WANT TO BUY CBCT: WHAT ARE THE KEY QUESTIONS TO ASK?
Like all purchases for your practice, wheth-er to buy a CBCT system should be a well-grounded business decision. The initial cost vs the price you can charge per scan is just the first step in deciding whether purchasing a CBCT system is a sensible business decision. While there are dental codes for CBCT, this does not mandate that insurance companies will actually pay for the procedure. Many of the reasons for imaging will be considered cosmetic and will also fall outside medical insurance reimbursement. Hence, if your patients are already paying cash for medical CT or CBCT scans, then you would be keeping those payments in house. Otherwise, you will be increasing fees or absorbing the costs of the procedure (and the purchase of the system) within your existing fee structure. Yes, you might also provide a service for other practitioners in your region; however, consider just how many of your competitors are likely to refer their patients to your center if there is even the slightest chance the patient will switch to your other services.
Also, be aware that regulations vary from region to region. Some states consider CBCT systems to be medical devices, and in some such states a certificate of need might be required for you to operate an imaging center. Before you buy, check with the local authorities to ensure that you will be permitted to run the CBCT system you intend to purchase. If the system is registered as a medical device, then it probably needs to be operated by either the dentist himself or a registered radiographic technician. Dental assistants are unlikely to be trained or credentialed to run a “medical” device.
Other major concerns should be the value added to your practice from this technology, the time and motion efficiencies, and also whether you are sufficiently trained and competent to read the full-tissue volumes that are imaged. You should also factor the time spent in reformatting images to specific templates and screening imaged volumes for unsuspected pathoses, as you are responsible for the recognition of disease represented throughout the imaged volume. If you are not comfortable with being held to the standard of a specialist in reading the imaged volumes, there will be an additional fee to pay for this service. Computer-aided diagnosis is in development but could be several years from validation and approval.
If you are still intent on buying a system, the first decision when selecting a CBCT system is the maximum field of view (FOV) that is required to image the volume of tissues necessary for your treatment plans. If you are an orthodontist or an oral surgeon—or wish to serve such practitioners—a large maxillofacial FOV is essential, but this will increase the price as the cost of detectors is highly size dependent. Should you be simply interested in dental implant planning, a restricted FOV can save perhaps 20% or more on the initial cost.
If you buy a full FOV system, you should insist on the ability to collimate to a shorter FOV that is sufficient for the diagnostic task in hand. A variable FOV permits minimization of the dose to the patient and also can significantly reduce computer reconstruction time for the acquired images. While exposure times are all relatively short, reconstruction time is generally dependent upon the FOV and the selected spatial resolution. The finer the resolution, the greater the reconstruction time; hence for high-resolution tasks, a restricted FOV is of importance in terms of time and motion ergonomics.
One decision point that is often over-emphasized by manufacturers is the maximum spatial resolution. In reality, most dental tasks require no smaller isotropic voxel resolution than 0.3 mm to 0.4 mm, and these are the levels of resolution preferred by most add-on services. In any event, it should be remembered that the finest spatial resolution proven by static test objects or cadaver specimens is not necessarily achievable in living individuals unless those individuals can be kept absolutely still. The ability of the cephalostat to hold the head still is of paramount importance in maximizing ef-fective spatial resolution. Speed and smoothness of motion during acquisition are additional factors impacting on effective resolution.
When buying a CBCT system, one should consider the way in which images will be stored and communicated. If you wish to have hard copies, then a diagnostic-quality printer for paper or transparency printouts can add to initial costs and also the cost of supplies. Medical-quality image printers can cost up to several tens of thousands of dollars. The alternative is to supply images in virtual format for reading on the computer monitor. With this in mind, the Next Generation i-CAT dataset output to i-CAT Vision is notable. The formatted dataset can be burned to CD-R and provides a free, fully interactive program viewer. All CBCT systems do permit DICOM image output that can be read by a variety of other software options; however, the referring practitioner usually needs to purchase such viewing software.
CBCT APPLICATIONS
The ADA Education in the Round session demonstrated the live acquisition of images on selected patients, reconstructions possible with the CBCT vendor’s software, and the export from each system of standardized DICOM format image datasets. These datasets were transported locally using CD-R and flash memory. Dr. Miles demonstrated that all datasets could be interoperated within Vworks/Accurex (Cybermed, Seoul, Korea). Making a careful review of all image sets for the presence of pathologic processes, he discovered numerous reportable conditions including calcifications within the brain of two of the eight subjects examined, and concha bullosa in three patients in succession. He emphasized the need for practitioners who purchase CBCT systems to systematically scan the imaged volumes for such pathoses and, where not comfortable to do so, to refer the image volumes for examination by a specialist in oral and maxillofacial radiology.
Virtual Models
Image data sets were also transferred for virtual model production using SimPlant master software (Materialise Dental Inc, Glen Burnie, MD) courtesy of 3D Diagnostix (Boston, MA). This transfer was accomplished via secure ftp and Simplant re-constructions were returned in less than an hour (Figure 2). From personal practice experience, the normal time for completion of conversions by 3D Diagnostix is within 2 to 3 hours after the company is notified of DICOM dataset upload.
Images such as these are valuable in assessing in 3-D the available bone height above the canal when implant planning is needed. An example of a case (not imaged at the ADA session) where such planning was not effected before implant placement is provided to show why CBCT is very important for planning dental implant placement (Figure 3). In this case, the mandibular canal was traced using the export of the DICOM dataset to Dolphin 3D software (Dolphin Imaging, Chatsworth, CA). The third dimension is precisely achieved by selecting a panoramic slice of just 1 voxel in thickness and then adjusting the reference image to maximize mandibular canal width and clarity.
Unfortunately, in this case the practitioner ordered the CBCT service after placing two implants, one into the anterior loop of the mental foramen and the other through the mandibular canal. This resulted in loss of sensation in the lower lip on the side concerned. In the authors’ opinion, using 3-D imaging such as CBCT before implant placement should be considered the required standard of care.
During the first two Education in the Round sessions, photographs were also made on each patient using the 3dMD camera system with the images ported to the 3dMDvultus™ Software Platform. 3dMD images are acquired by an array of cameras in 1.5 milliseconds to eliminate all motion. This reconstruction can be rotated to any view angle within the 3dMDvultus software provided with the system. This type of imaging can be used for orthodontics and orthognathic surgery planning and treatment simulations. Because of time constraints, the demonstration of the fusion of photographic datasets to CBCT data from each of the four CBCT systems was carried out at a subsequent session. At that session, the primary author was the “live” patient for the purposes of acquiring photographic images and fusing these to a CBCT dataset that had been acquired earlier for diagnostic purposes (Figure 4; Figure 5; Figure 6).
For excellence in 3-D reconstruction of image datasets for general viewing as well as for orthodontic assessment, two leading software systems were used; namely Dolphin Imaging and InVivoDental™ (Anatomage, San Jose, CA). Figure 7 demonstrates some of the segmentation strengths of these excellent programs. In talking with several of the CBCT manufacturers, it was evident that they were happy to have these two companies provide add-on services to supplement those they could provide with their basic image acquisition and display software.
Panoramic reconstructions are the basis for selecting jaw cross-sections for implant planning, but have now been refined for more precise 3-D anatomic representations than are possible with traditional panoramic radiographic systems (Figure 8).
The power of segmenting tissues is amply demonstrated in Figure 9. This is an Anatomage segmentation of the left side of one of the patients imaged live at the ADA Annual Session. It clearly demonstrates the airway and facial surface profile in white while indicating bone in orange and the mandibular canal in red. In the authors’ opinion, the achieved image quality rivals that found in the best anatomy texts.
It is also possible now using CBCT to prepare virtual study models to assess the positions of the teeth (Figure 10). Unlike traditional study models made of plaster or stone, it is possible to show the tooth roots as well as their crowns. The precision is not yet sufficient for making dyes for prosthodontics to construct fixed crowns-and-bridges. This would need at least an order of magnitude more accuracy than is possible with the finest spatial resolution currently achievable using CBCT.
Physical Surgical Positioning Stents and Models
For implant planning, image sets were processed by n-Sequence (Reno, NV) a company that provides services using VIP Virtual Implant Placing software (Implant Logic, Cedarhurst, NY); ImplantMaster (iDent, Ft Lauderdale, FL); and EasyGuide (Keystone Dental, Burlington, MA). Dr. Schiff also demonstrated cases processed by Nobel Biocare’s Procera® (Yorba Linda, CA). From such software and systems it is possible to manufacture surgical positioning stents to assist in implant placement. We refer readers to our June 2007 article, where this process was described in detail.
Image data sets were also sent to Imtec Corporation for 3-D model printing and to Biomedical Modeling, Inc (Boston, MA) for stereolithographic production of models (Figure 11). The time taken to manufacture such anatomic models precluded this being achieved live during the ADA Annual Session, so it was simulated using previously submitted datasets for each of the four CBCT systems demonstrated. Subsequently, models have been constructed on datasets submitted from the live show. It usually takes a day or two for actual production, and given transportation to and from the company making the models, a 1- to 2-week turnaround can be expected.
CONCLUSION
It should be obvious that CBCT is here to stay and will have a tremendous impact on the practice of all disciplines within dentistry. The use of 3-D imaging for planning dental implant placement is rapidly becoming the standard of care. If complications occur in the absence of such images, the practitioner placing the implants will likely have little defense when subjected to the legal process. This does not mean that you must own a CBCT system if you place implants; however, you should be referring your patients for 3-D imaging and, as CBCT results in an order of magnitude less radiation than medical fan beam CT, you will be best serving your patients if you select CBCT.
For dental implant planning, any approved CBCT system can be used. To minimize the patient-radiation dose it is best to choose either a large FOV unit with variable collimation or a CBCT that inherently has a small FOV. For purposes other than local evaluation of the jaws, you will need to select a system with a large FOV. If you expect to run an imaging center with referrals from diverse specialties, this is undoubtedly the best choice. Orthodontics and maxillofacial surgery are examples of disciplines where a large FOV that encompasses most of the head is preferred.
While not yet a critical standard of care for cephalometrics, it is likely that with appropriate evidence the move will be toward 3-D imaging for planning orthodontic treatment. Certainly, simulations of the affects of orthodontics and orthognathic surgical procedures are best performed with 3-D image datasets. Further, CBCT can provide adequate resolution to replace the traditional plaster study model, and thereby remove the need for the relatively unpleasant, time-consuming, and costly procedure of taking impressions. It can be expected that there will be growth in the numbers of CBCT systems available to US dentists over the next 6 to 12 months, and also a growth in the quality and the numbers of associated software packages and allied services.
 | 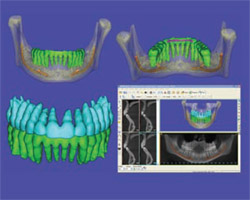 | |
| Figure 1 The Education in the Round live demonstration of four cone beam CT systems. | Figure 2 SimPlant reconstructions of the DICOM image dataset from the Next Generation i-CAT. The mandible is demonstrated in the top two images with color-coding of the teeth (green) and mandibular canal (orange). The lower images show the dentition with the maxillary teeth coded (blue). | |
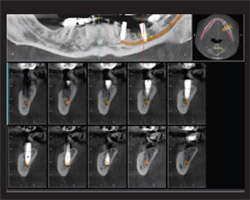 | 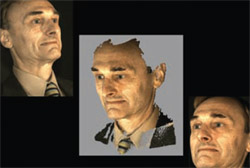 | |
| Figure 3 Images reconstructed with Dolphin 3D technology. The upper (left) image is a simulated panoramic view, the upper (right) image is the axial slice used to generate the panoramic contour, and the lower views are cross-sectional reconstructions through an implant placement site in the lower jaw. | Figure 4 The upper and lower images are examples of the original photographs and the center image (with gray surround) is a 3-D photographic reconstruction. | |
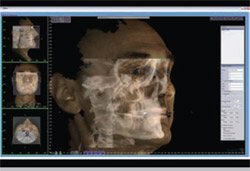 | 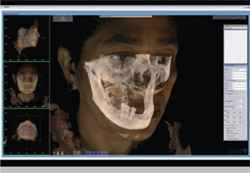 | |
| Figure 5 Fusion of a 3dMD photographic dataset to a corresponding Next Generation i-CAT CBCT dataset. | Figure 6 Fusion of a 3dMD photographic dataset to a corresponding NewTom VG CBCT dataset. | |
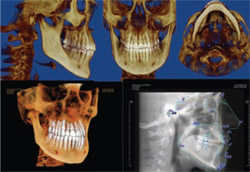 |  | |
| Figure 7 Reconstructions of a Next Generation i-CAT CBCT dataset using Dolphin 3D (upper three images) and Anatomage (lower two images) technology. | Figure 8 InVivoDental reconstructions of a Next Generation i-CAT CBCT dataset demonstrating panoramic reconstruction both in traditional form (lower right) and as a 3-D volume that can be rotated (upper image). | |
 | 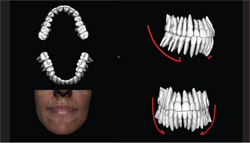 | |
| Figure 9 InVivoDental reconstructions of a Next Generation i-CAT CBCT dataset demonstrating the hard tissue, airway, and facial profile. | Figure 10 InVivoDental reconstructions of a Next Generation i-CAT CBCT demonstrating the production of virtual dental models from segmentation of the teeth. | |
 |  | |
| Figure 11 Stereolithographic models made from Iluma and NewTom DICOM image datasets provided to Biomedical Modeling, Inc, via secure ftp. The teeth and mandibular canals are colored red in the process used by this company. | ||
| About the Authors | ||
 Allan G. Farman, BDS, PhD, MBA, DSc Allan G. Farman, BDS, PhD, MBA, DSc Professor of Radiology and Imaging Sciences Department of Surgical and Hospital Dentistry University of Louisville Louisville, Kentucky Diagnostic Maxillofacial Imaging University Associates Louisville, Kentucky | ||
Claudio M. Levato, DDS William C. Scarfe, BDS, MS James Mah, DDS | ||

