
Preservation of Surrounding Tissue With New Instrumentation
An ever-heightened esthetic standard and the need for the predictable stabilization of immediately placed implants have created a focus on the preservation of the existing intraoral architecture to provide support for the final prosthesis before and during the extraction phase of the tooth. Previously, the method taught in dental schools—and almost universally employed—for eliminating the fibrous attachment and expanding the osseous support of the tooth was bucco-lingual luxation using elevators and forceps.
The forces applied using standard elevators and forceps cause this technique to be fraught with complications: fracture of the tooth or root, surgical removal of bone for greater access, and necrosis resulting from traumatic force. Karl Schumacher (Southampton, PA) has introduced a new surgical protocol using apical instrumentation that allows for the preservation of the hard and soft tissues by focusing on occlusal movement of the tooth during extraction. This technique allows for the removal of most broken-down teeth using a closed (non-flap) procedure. This technique also eliminates the retentive factors that hold a tooth in place in a specific, logical sequence. These factors include the periodontal ligament (PDL), root anatomy, and multi-rooted teeth. Within the scope of this technique, Schumacher Periotomes are instruments designed to cut the PDL attachment of the root, effectively reducing the actual attachment of bone to the root. Schumacher ProximatorsTM are then used to further eliminate the PDL and create slight lateral compression of the bone in the mesio-distal areas. Finally, Apical Retention Forceps, designed to access the limited contact area created by the other instruments, are then used for final delivery of the tooth.
CASE PRESENTATION
A 71-year-old man presented for extraction of teeth Nos. 13 and 14. The preoperative radiograph (Figure 1) showed a close relationship between the apex of the roots and the sinus floor. The patient was reluctant to undergo sinus augmentation, and little bone was available to support the proposed implants. The teeth had previously undergone root canal therapy as well as full-coverage restorations. There was excessive mobility on teeth Nos. 13 and 14. There was not enough bone vertically that, if any were to be lost in the extraction, there would not be enough bone to support the implant, especially concerning the No. 14 area. Tooth No. 15 also was not supportive enough to support a new bridge as an abutment. Implants would be the only way to avoid a removable prosthesis. Ideally, these teeth would be removed in a closed procedure, without compromising the sinus floor and with minimal or no bone loss. After preservation of the bony ridge during extraction, the socket could be grafted and left to heal for an appropriate time, or an implant could be placed immediately, provided the correct support was available.
PERIOTOMES
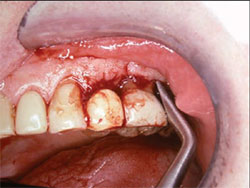
Initially, a Schumacher Periotome was inserted into the PDL on the mesio-buccal aspect and worked circumferentially around the tooth with slight apical pressure (Figure 2). The thin blades of the instrument were rocked in a direction parallel to the root surface to “walk” the tip around the teeth, making further apical progress with each reinsertion. Once a significant portion of the ligaments were severed using the straight blade, the socket expander end was used with a slight wheel-and-axis motion to laterally expand the crestal bone (Figure 3). This expansion facilitated the insertion of the other instruments into the PDL space.
PROXIMATORS
Next, an angulated Schumacher Proximator was used on the distal portion of tooth No. 14 (Figure 4), wedging the bone in a mesio-distal direction, thereby creating a larger area for an occlusally directed extraction. Some expansion of the surrounding bone can be beneficial in the delivery of teeth, as curvature of the roots or undercuts caused by the undulation of the root surfaces might impede the roots from escaping the bone along the best path of delivery. Originally, the thin buccal or labial plate was often the only available bone at which to direct expansion efforts; however, the Proximators are angled in such a way as to take advantage of thicker and more pliable interproximal bone to create space for delivery. Also, the angulations of the Proximators afford the ability to create space in the bone on previously unattainable aspects, while the strength of the tips enables insertion more apically than the Periotomes.
As in the case presented, multi-rooted teeth create a challenge because the roots are rarely parallel to one another. The natural anatomy of the trifurcated root works to enhance retention and spread functional stress to the underlying bone. Sectioning multi-rooted teeth eliminates this retentive capacity, and allows each root to be removed individually. Multi-rooted teeth can also be sectioned, essentially creating the extraction of multiple single-rooted teeth. After sectioning, a Proximator is then inserted to expand the alveolus around each root, enabling each root to follow its own ideal path of delivery. They are then extracted in an occlusal direction as if they were single-rooted teeth.
APICAL RETENTION FORCEPS
After the initial application of the Periotomes and Proximators, teeth Nos. 13 and 14 were extracted using the Apical Retention Forceps (Figure 5). These forceps combine several modifications that enable a firmer purchase on the root surface of the tooth. The sharpened beaks of the forceps enable deeper apical progress to engage the crown and root structure. The parallel gouge design of the beaks is more anatomically correct, and assures multiple contact points during application, while the longitudinally cut serrations enhance the grip on the tooth during extraction. A more apical placement on the root structure, greater conformity to the true shape of the tooth, and multiple contact points lessen the instance of the forceps slipping and damaging any surrounding structures. Because of the elimination of the PDL with the Periotomes, and the lateral expansion of the bone using the Proximators, the Apical Retention Forceps are able to deliver the tooth and root from the alveolus intact, eliminating the incidence of root fracture and full surgical involvement.
CONCLUSION
This article has reviewed the extraction of multi-rooted teeth and successful placement of implants in an atraumatic procedure where the patient could ill afford additional bone loss (Figure 6). Karl Schumacher’s apical instrumentation gives the dentist a controlled, positive delivery of the retained root structure and protection of the hard and soft tissues, with reduced chair time and less trauma for the patient.
The preservation of a ridge that will have extraction(s) performed should be considered before the extraction. After initial planning, choosing the best techniques and instruments to accomplish the task is essential. By progressively using all three of these new instruments (Periotomes, Schumacher Proximators, and Apical Retention Forceps), an occlusal delivery of the indicated teeth and roots can now be safely and predictably achieved, all while preserving the hard and soft tissues of the bony ridge.
The case shown presents the ideal surgical outcome; the placement of implants immediately after an extraction, where initial stability is enhanced because of the preservation of the natural support structures as the result of the application of advanced surgical instrumentation and techniques.
ACKNOWLEDGMENT
This article was written by David L. Hoexter, DMD, clinical professor in the Department of Periodontics at Temple Uni-versity, Philadelphia. His private practice in New York City is limited to periodontics, esthetics, and implantology.
For more information, contact:
Karl Schumacher
1-800-523-2427
www.karlschumacher.com
DISCLAIMER
The preceding material was provided by the manufacturer. The statements and opinions contained therein are solely those of the manufacturer and not of the editors, publisher, or the Editorial Board of Inside Dentistry. The preceding is not a warranty, endorsement, or approval for the aforementioned products or services or their effectiveness, quality, or safety on the part of Inside Dentistry or AEGIS Communications. The publisher disclaims responsibility for any injury to persons or property resulting from any ideas or products referred to in the preceding material.
 |  | |
| Figure 1 When the patient presented for extraction of teeth Nos. 13 and 14, the preoperative radiograph showed a close relationship between the apex of the roots and the sinus floor. | Figure 2 The Schumacher Periotome was inserted into the PDL on the mesio-buccal aspect and worked circumferentially around the tooth with slight apical pressure. | |
 |  | |
| Figure 3 The socket end of the Schumacher Periotome was used with a slight wheel-and-axis motion to laterally expand the crestal bone after a significant portion of the ligaments were severed with the straight blade. | Figure 4 An angulated Proximator was used on the distal portion of tooth No. 14 to wedge the bone in a mesio-distal direction. | |
 |  | |
| Figure 5 Teeth Nos. 13 and 14 were extracted using the Apical Retention Forceps. | Figure 6 The final radiograph showing the end result of the extraction of the multi-rooted teeth and successful placement of implants in an atraumatic procedure. |

