

An Innovative Restorative Option for the Maxillary Arch
Thomas Dudney, DMD
Dentists are constantly challenged to find the proper balance between function and esthetics when restoring the anterior maxilla. Both metal-ceramic and all-ceramic restorations can present suitable options for treating this region, provided the clinician uses a proper treatment protocol. This article demonstrates the author’s approach for achieving longevity and esthetics in the replacement of existing crowns.
Dental professionals are continuously exposed to new materials, techniques, and outlooks on patient care—particularly in esthetic dentistry. Although innovative technologies for fabricating restorations, such as alumina or zirconia ceramics and computer-aided design/computer-aided manufacturing, have increased the treatment options available to clinicians and their patients, porcelain-fused-to-metal restorations continue to represent a suitable course of treatment in many situations.
Throughout history, gold dental restorations have a proven track record regarding strength and durability. Recently, a metal-composite material (Captek™, Precious Chemicals Company, Inc, Altamonte Springs, FL) has been introduced from this foundation, which provides dentists with an accurate restorative material that has demonstrated resistance to bacteria accumulation, durability, and esthetics. Restorations fabricated of this biocompatible metal-composite material can be designed with virtually any type of margin, for crowns and three-unit fixed partial dentures, and particularly for masking dark substructures.
Esthetics is a major component of dentistry. Using current restorative materials, esthetics need not compromise strength and durability. This article demonstrates a clinical protocol for achieving natural esthetics and function in a patient who desired esthetic enhancement of preexisting anterior restorations.
Diagnosis and Treatment Plan
A 50-year-old woman presented with a chief complaint of her maxillary anterior teeth impinging on her lower lip. The patient’s medical history was negative and the periodontal condition was stable. A clinical examination revealed healthy temperomandibular joints with no muscle soreness or tenderness. The posterior teeth had been previously restored with full-coverage crowns, but radiographs were negative. Her maxillary and mandibular teeth from premolar to premolar had been restored approximately 3 years previously with porcelain laminate veneers to treat excessive wear of the anterior teeth. At the examination, it was determined that her difficulties might be attributed to overclosure as a result of a loss of vertical dimension. The patient also had had the length of her maxillary anterior veneers adjusted in an attempt to alleviate the pressure to her lower lip, resulting in a shortening of the incisal edges and a decrease in the amount of tooth display in her smile (Figure 1).
A treatment plan was presented requiring the restoration of the entire maxillary arch to open the bite and allow for an increase in incisal length. All-ceramic restorations were chosen for the anterior six teeth for maximum esthetics and the ability to bond etched porcelain. On the posterior teeth, porcelain-fused-to-metal composite (Captek) restorations were chosen for strength and durability as well as marginal fit and excellent tissue compatibility. Additionally, the warm gold color of the substructure would provide esthetics for this region and would permit them to be cemented conventionally.
Treatment
The initial step was to make impressions for study models, perform a face-bow transfer (Rotofix, Jensen Industries, North Haven, CT), take a centric relation bite using a lucia jig (Great Lakes Prosthodontics, Tonowanda, NY), and take a set of photographs (eg, full-face, smile, and retracted views of the teeth). This information was sent to the dental laboratory where a diagnostic wax-up, preparation guides, and a putty matrix (Sil-Tech, Ivoclar Vivadent, Amherst, NY) of the wax-up was fabricated. After communicating with the ceramist, it was determined that by opening the bite 1 mm posteriorly, the patient would gain approximately 2.5 mm to 3 mm anteriorly, which would be adequate to satisfy the restorative needs.
During the preparation appointment, all of the previous restorations were removed and the teeth were reprepared. After the preparations were completed, provisional restorations were made using the putty matrix with Luxatemp® shade B1 (Zenith/DMG, Englewood, NJ), at the new vertical dimension determined by the diagnostic wax-up, trimmed, and set aside (Figure 2A). The provisionals for the central incisors were separated and placed on the teeth to serve as an anterior stop at the proper vertical dimension. The bite registration material (LuxaBite™, Zenith/DMG) was then injected bilaterally and the patient was gently manipulated to closure with the condyles fully seated and the mandibular anterior teeth in light contact with the central incisor provisionals. In addition to this centric relation bite registration, a face-bow transfer, stick bite for horizontal reference (Figure 2B), and a photograph of the stump shade were taken (Figure 2C). After the polyvinyl siloxane impression was made, the teeth were cleaned and the provisional restorations were seated with LuxaFlow™ (Zenith/DMG).
After final contouring of the provisionals, the occlusion was adjusted to ensure equal intensity centric stops, anterior guidance within the patient’s envelope of function, and posterior disclusion in all excursive movements. Although the patient was still anesthetized, she stated that her mouth already felt better. The incisal length of the central incisors, which was 11 mm, was recorded and photographs as well as an impression of the provisional restorations were taken to aid in laboratory communication.
Two days later, the patient was seen for a postoperative visit at which time additional pictures were taken to visualize the relation of the teeth to the lips and to use phonetics to check the length and incisal edge position. The patient was satisfied with her improved appearance and comfort. Minor adjustments were made, and the patient’s postoperative instructions were reinforced.
During the insertion appointment, the provisionals were removed, and the preparations were cleaned with hydrogen peroxide. The definitive restorations were tried for fit and then prepared for cementation (Figure 3). The definitive Captek restorations (Figure 4) would be conventionally cemented in the posterior region, thereby avoiding the need to perform isolation with a rubber dam. After the posterior restorations were cemented and cleaned of excess cement, the anterior segment was isolated with a rubber dam and the six porcelain laminate veneers were bonded in place with luting cement (Appeal+1, Ivoclar Vivadent) (Figure 5). After clean-up, the occlusion was checked, minor adjustments were made, and the restorations were polished (Figure 6). The patient was scheduled for a postoperative visit, at which time the occlusion was rechecked and the length and incisal edge position was verified phonetically (Figure 7A; Figure 7B; Figure 7C and Figure 8).
Conclusion
Because of the increasing desire for esthetic restorations, research facilities and development departments are working to create “the perfect ceramic material” which can deliver optimal strength and esthetics. In many cases, however, it is simply unacceptable to sacrifice durability and strength for esthetics. When strength is a primary concern, gold and/or porcelain-to-gold restorations are still the proven choice. In this case, porcelain-fused-to metal Captek restorations proved to be an ideal treatment material that delivered several benefits, resulting in a durable esthetic restoration, and a satisfied patient.
Acknowledgment
The author would like to acknowledge his gratitude to Jurim Dental Studio, Great Neck, New York, for the fabrication of the restorations.
 |  | |
| Figure 1 A 50-year-old woman presented with a chief complaint of her maxillary teeth impinging on her lower lip. | Figure 2A The putty matrix with Luxatemp. | |
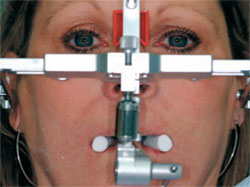 |  | |
| Figure 2B A face-bow transfer and stick bite were taken for horizontal reference. | Figure 2C Photograph of the stump shade for reference. | |
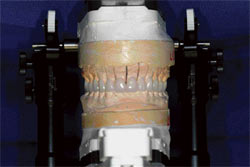 |  | |
| Figure 3 Definitive restorations were prepared for cementation. | Figure 4 Captek restorations were cemented posteriorly. | |
 |  | |
| Figure 5 After the restorations were cemented and cleaned of excess cement, the porcelain veneers were bonded in place with luting cement. | Figure 6 After clean-up, the occlusion was checked and the restorations were polished. | |
 |  | |
| Figure 7A | Figure 7B | |
 Figure 7C |  | |
| Figures 7A through 7C The esthetic metal-ceramic restorations were well integrated upon the postoperative evaluation. | Figure 8 Postoperative view of the patient's smile. The patient was pleased by the enhanced function and esthetics. | |
| About the Author | ||
 Thomas Dudney, DMD Thomas Dudney, DMD Private Practice Birmingham, Alabama | ||

