

Endodontic Retreatment Techniques
Samuel Kratchman, DMD, and Mian Iqbal, DMD
Unfortunately, no dental procedure comes with a 100% guarantee. Although there have been vast technological improvements in the field of endodontics during the last several years, one must still accept that a certain number of endodontic cases will fail and require retreatment.1-4 The purpose of this article is to discuss some of the various techniques for successful retreatment.
Before beginning a retreatment, one must carefully construct a treatment plan and understand the limitations and possible complications of the procedure.5-9 Some teeth are helpless and will require extraction (Figure 1).
There are certain instruments that should be a part of the armamentarium for those cases that are retreated. For the removal of gutta percha as well as the new resin-reinforced gutta percha, heat and solvents (ie, chloroform), LA Axxess burs (SybronEndo, Orange, CA), gates glidden drills, and nickel titanium rotary files (at 1200 rpm) can be used.10-13 With gutta percha carrier systems such as Thermafil® (Dentsply International, York, PA) in addition to the above mentioned mechanisms, the braiding technique can also be used. In this technique, the gutta percha is bypassed on multiple sides and then two or more Hedstrom files are threaded past the Thermafil carrier. The handles of the two Hedstrom files are then twisted to remove the gutta percha/Thermafil as a unit.14,15 Once the gutta percha has been removed, it is important to use an apex locator to determine the “new” working length. There are often periapical radiolucencies with teeth requiring retreatment, and the radiographic apex will not be the same as the actual clinical apex, especially when resorption is present (Figures 2A and 2B). Therefore, the use of an apex locator is critical for determining the apical extent of the obturation.
Retreatments often require the removal of metal posts, pins, silver points, or other obstructions.16 There are several types of forceps available to remove the obstructions (eg, steiglitz, peete, hemostats) (Figures 3 and 4). A custom instrument can be made by cutting a groove into the tip of a spoon excavator, which gives it the appearance of a snake’s tongue (Figure 5). This can be extremely helpful in elevating out a pin once it has been loosened with ultrasonics.
The first step in the removal of posts and pins is the use of diamond-coated ultrasonic tips (Obtura Spartan, Fenton, MO) (Figure 6). These tips are used at a low-frequency setting without water. The assistant should blow a fine stream of air, which removes excess debris and reduces the heat generated by the tips. They are designed to efficiently remove the cement around a post or pin, helping to loosen it (Figure 7). These diamond-coated ultrasonic tips are not designed to purposefully vibrate directly against the metal obstruction.
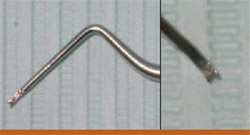
Another instrument helpful in loosening a post is a Rotopro (Ellman International, Inc, Hewlett, NY) (Figure 8). These are noncutting fluted stainless steel instruments used with water in a high-speed hand piece. By rotating around the post in a counter-clockwise direction, the cement is chipped away and the threads of the post will start to unwind.
By using the above-mentioned techniques, endodontic retreatments can more predictably and efficiently be performed. Careful case selection and experience will allow the clinician to re-treat cases with a high success.
Case No. 1
The patient had previous root canal with a post-and-crown therapy on the maxillary bicuspid (tooth No. 13). In this case, the first choice might have been apical surgery, which would have been a straightforward procedure. However, after removing the post and inspecting the access, it was discovered that not one but two canals were missed from the first root canal treatment. The final radiograph shows the three treated canals. In retrospect, apical surgery would have failed because of the two untreated canals (Figures 9A;9B; 9C).
Case No. 2
This patient has previous endodontic treatment on the maxillary molar (tooth No. 14) and presented with a lesion around the apex of the palatal root as well as slightly lateral on the root. On removal of the gutta percha using a combination of gates glidden burs and rotary nickel titanium files, it was discovered that there was an apical bifurcation of the canal. To successfully obturate this case, the first master cone of gutta percha was placed into the bifurcation and then burned down with a System-B (SybronEndo) to within approximately 2 mm of the working length. This made room for the placement of a second gutta percha cone in the main palatal canal, which was then burned down and back-filled with Obtura III (Obtura Spartan, Fenton, MO) (Figures 10A; 10B; 10C; 10D).
Case No. 3
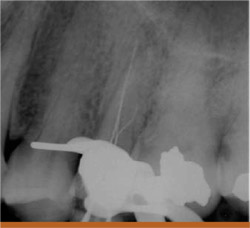
This patient had a maxillary bicuspid (tooth No. 12) with a separated instrument in one canal. The technique used to remove the broken instrument involved a piece of 25-gauge irrigating needle, which formed a hollow tube. Once the file was moved away from the inner wall of the canal using diamond and titanium ultrasonic tips, the tube-shaped irrigating needle was positioned over the coronal end of the separated file. The end of the broken file that was within the hollow tube was then wedged against the inner wall of the hollowirrigating needle by inserting a #40 Hedstrom file through the other endof the hollow tube and removing the separated file/tube and Hedstrom asone unit. With the canals clear, theretreatment could be readily completed (Figure 11).
Conclusion
Although root canal treatment is becoming a more predictable procedure with a high success rate, there are still a certain percentage of cases that fail, whether a result of leakage, procedural mishaps, missed canals, or unusual canal anatomy. With the proper armamentarium and knowledge of several varieties of treatment, one can perform root canal retreatments with great success and maintain the patient’s natural tooth.
References
1. Chong BS, Pitt Ford TR. Endodontic retreatment. 1: indications and case selection. Dent Update. 1996;23(8):320-328.2. Wong R. Conventional endodontic failure and retreatment. Dent Clin North Am. 2004;48(1): 265-289.
3. Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phases I and II: orthograde retreatment. J Endod. 2004;30(9):627-633.
4. Paik S, Sechrist C, Torabinejad M. Levels of evidence for the outcome of endodontic retreatment. J Endod. 2004;30(11):745-750.
5. Chong BS, Pitt Ford TR. Endodontic retreatment. 2: methods. Dent Update. 1996;23(9):384-390.
6. Pagonis TC, Fong CD, Hasselgren G. Retreatment decisions—a comparison between general practitioners and endodontic postgraduates. J Endod. 2000;26(4):240-241.
7. Mounce R. Endodontic retreatment possibilities: evaluation, limitations, and considerations Compend Contin Educ Dent. 2004;25(5):364-368.
8. Ruddle CJ. Nonsurgical retreatment. J Endod. 2004;30(12): 827-845.
9. Peikoff MD. Treatment planning dilemmas resulting from failed root canal cases. Aust Endod J. 2005;31(1):15-20.
10. Sae-Lim V, Rajamanickam I, Lim BK, et al. Effectiveness of ProFile .04 taper rotary instruments in endodontic retreatment. J Endod. 2000;26(2):100-104.
11. Imura N, Kato AS, Hata GI, et al. A comparison of the relative efficacies of four hand and rotary instrumentation techniques during endodontic retreatment. Int Endod J. 2000;33(4):361-366.
12. Valois CR, Navarro M, Ramos AA, et al. Effectiveness of the ProFile.04 Taper Series 29 files in removal of gutta-percha root fillings during curved root canal retreatment. Braz Dent J. 2001;12(2):95-99.
13. Mounce R. Current concepts in gutta-percha removal in endodontic retreatment. NY State Dent J. 2004;70(7):32-35.
14. Wolcott JF, Himel VT, Hicks ML. Thermafil retreatment using a new “System B” technique or a solvent. J Endod. 1999;25(11): 761-764.
15. Guess GM. Predictable Therma-fil removal technique using the system-B heat source. J Endod. 2004;30(1):61.
16. Foroughi K, Sedaghat-Zandi A, Friedman S. Post removal techniques used in nonsurgical endodontic retreatment. NY State Dent J. 1999;65(5): 28-29.
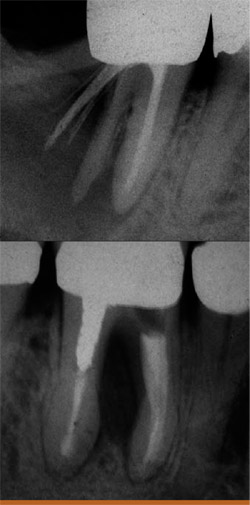 |  Figure 2A Preoperative radiograph of a tooth with large periapical lesion and apical resorption.  | |
| Figure 1 Two teeth that needed to be extracted because of split root and strip perforation. | Figure 2B At the 7-month recall, the bone is shown to be healing around the apex. | |
 |  | |
| Figure 3 Steiglitz forceps with different angles. | Figure 4 Samples of other forceps, including Peete forceps, micro-forceps, and hemostats. | |
 | ||
| Figure 5 A custom-made "snake-tongued" spoon excavator. | ||
 |  | |
| Figure 6 Diamond-coated Spartan CPR Ultrasonic tips and the Spartan Ultrasonic unit. | Figure 7 Example of the CPR ultrasonic tip being used to remove cement around a post. | |
 |  | |
| Figure 8 The Rotopro stainless steel bur with a noncutting fluted surface. | Figure 9A Preoperative radiograph of a maxillary bicuspid with a post and crown and a periapical lesion. | |
 |  | |
| Figure 9B A working-length radiograph shows three canals. | Figure 9C The postoperative radiograph shows the three filled canals. | |
 Figure 10A The preoperative radiograph of a maxillary molar with lesions around the palatal apex.  Figure 10B The file going into apical bifurcation.  Figure 10C Two master cones were placed in the palatal canal.  Figure 10D The final radiograph. |  Figure 11 The technique of fitting a hollow needle tip over the separated file and wedging it in place with a Hedstrom file. A The separated file is removed by wedging it inside a hollow needle tip with a 40 Hedstrom. B Lower magnification of the unit after separated file removal. C 40 Hedstrom, hollow needle tip, separated file. D Preoperative radiograph showing both canals and the separated file. E Straight-on preoperative radiograph. F Radiograph after file removal and completion of retreatment. | |
| About the Authors | ||
 Samuel Kratchman, DMD Samuel Kratchman, DMD University of Pennsylvania Department of Endodontics Philadelphia, PA Private Practice Exton, PA | ||
 Mian Iqbal, DMD Mian Iqbal, DMD University of Pennsylvania Department of Endodontics Philadelphia, PA | ||

