
Clinical Success of Reciprocating One-Visit Endodontic Cases
The overall endodontic treatment is comprised of many separate techniques and procedures. Each one of these techniques and procedures can be considered a subdivision of the whole, a link in the chain of treatment. These separate links can be divided into diagnosis, anesthesia, isolation, access, finding canals, canal measurement, instrumentation, irrigation, obturation, and temporization. Every step is interdependent and no one is more important than any another in achieving clinical success. Each procedure paves the way for the next step in the endodontic treatment. Over the years many new techniques in each of these steps have been advocated to achieve clinical success. Instrumentation, irrigation, and obturation have received particular attention in the last 15 years. Many of these new techniques and materials have been advocated without substantial in vitro or clinical testing. The outcome of inadequate testing of these materials and techniques can be catastrophic. The recall and discontinued use of the endodontic obturation material “hydron” in the late 1980s is an example. Because the primary goal of all treatment is clinical success, we hold that as the gold standard.
Since 1998 we have been doing endodontics primarily in one visit using the SafeSiders endodontic reamers and technique (EDS, South Hackensack, NJ). We have been achieving 3D obturation of the canal with a single gutta percha cone, the bidirectional spiral, and EZ-Fill cement (EDS). Irrigation and disinfection has been achieved using sodium hypochlorite, 17% EDTA (Pulpdent, Boston, MA) and 2% chlorhexidine (Vista, Racine, WI). We have found this combination of materials and techniques to be very effective. In clinical studies we have reported a 94.1% success rate.1-3
After diagnosis, anesthesia, access preparation with the Pulpout bur (EDS), and canal measurement (Endex, Osada, CA) are achieved, we instrument the canal with the engine-driven, reciprocating SafeSiders reamers. Reciprocation of endodontic instruments is an old technique first introduced in the late 1970s. The newest iteration of this technique uses instruments that are, for the first time, specifically designed to take advantage of this movement. The SafeSider instruments, both stainless steel and titanium, have a flat side that creates a chisel-like cutting edge well suited for the reciprocal movement of the Endo-Express handpiece (EDS) (Figure 1).
The instrumentation technique is easy to understand and use. Inexpensive stainless steel instruments, with the smaller sizes being extremely flexible, are used in the reciprocating handpiece to create the glide path to the apex (Figure 2). After a size 20 (yellow) instrument is used, a #2 peeso is used in a crown-down manner to within 6 mm of the apex, if possible. Opening up the coronal aspect of the canal with the peeso lets each succeeding instrument cut only at its apical 1 mm to 3 mm, resulting in little stress placed on the instrument and very fast canal preparation. Once the peeso is used then the canal is widened to a #30 or #35 to the apex using the reciprocating handpiece. A #40 stainless steel reamer is then used 1 mm short of the apex. To gain the final flare and shape of the canal, 2 NiTi instruments in the reciprocating handpiece are used. First the 30/04 NiTi is used in the handpiece to the apex followed by the final instrument, the NiTi 25/08. The tip of the 25/08 is smaller than the 30/04; therefore, it does notcut at the apex but merely increases the taper of the canal. Because we are reciprocating (30 to 45 degrees) and not rotating the NiTi instruments, the NiTi instruments will not thread into nor bind in the canal with all the concomitant problems.
During instrumentation we are always irrigating. We use sodium hypochlorite 5.25% from instruments #8 through #40. We suction out the old irrigant and place new irrigant between each file size change. When we instrument with the NiTi instruments we change the irrigating solution to 17% EDTA. This is done to remove the smear layer. Removal of the smear layer does 2 things: it opens the tubules to allow disinfection and reduction of the bacterial count; and it lets the endodontic sealer penetrate into the tubules and creates a better seal. This has especially been shown for epoxy sealers.
The EDTA is then washed out with either sterile water or anesthetic solution. This prevents precipitate formation with the next irrigant, 2% chlorhexidine. We leave the chlorhexidine in the canal for 2 minutes. Chlorhexidine does 2 things very well: it kills bacteria (even E faecalis for up to 12 weeks); and it promotes collagen stability for long-term bonding to dentin of epoxy-based sealers.
Once the chlorhexidine rinse has been accomplished we are ready to obturate the canals. We mix EZ-Fill sealer to cement consistency. We pick up cement with the bidirectional spiral and place it into the canal. We rotate the spiral at approximately 1,000 rpm. The spirals at the coronal end of the instrument push the sealer towards the apex. The apical 3 mm of spirals go in the opposite direction and push the cement coronally away from the apex. At the 3-mm level where the different spirals meet the cement is spun out laterally. This prevents sealer from being placed past the apex.
Once the canal is filled with sealer and the apical 3 mm to 4 mm of the prefitted gutta percha point has been coated with cement, the point is slowly placed to the measurement. As in all techniques, the sealer is what ultimately seals the canal. Figures 3 and 4 show examples of infected cases that have healed and withstood the test of time.
References
1. Musikant BL, Cohen BI, Deutsch AS. A two and a half year perspective of simplified endodontic techniques. Compend Contin Educ Dent. 2003;24(1): 930-942.2. Deutsch AS, Cohen BI, Musikant BL, et al. A study of one visit treatment using EZ-Fill root canal sealer. Pract Endod. 2001;4(3):29-36.
3. Deutsch AS, Cohen BI, Musikant BL, et al. Two year recall study for EZ-Fill Root Canal Obturation System. J Den Res. 2001;80:257(Abstract 1773).
This article was written by Allan S. Deutsch, DMD and Barry Lee Musikant, DMD.
For More Information
Essential Dental Systems
Phone: 1-201-487-9090
E-Mail: info@edsdental.com
Web: www.edsdental.com
 Figure 1 The SafeSider instruments have a flat side that creates a chisel-like cutting edge well suited for the reciprocal movement of the Endo-Express handpiece. 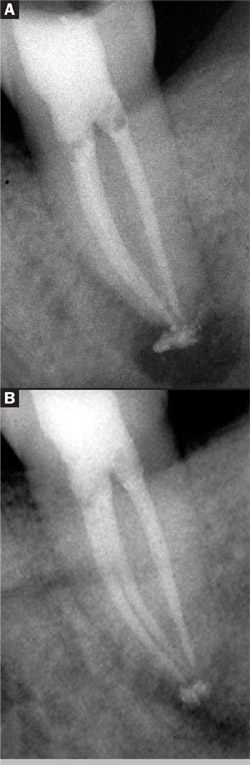 |  Figure 2 Inexpensive stainless steel instruments are used in the reciprocating handpiece to create the glide path to the apex.  | |
| Figure 4 (A) Endontics complete. (B) Postoperative healing at 1 year. | Figure 3 (A) Preoperative radiograph showing periapical radiotranslucency. (B) Endodontics complete. (C) 1-year postoperative image showing periapical radiotranslucency has healed. |

