You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
When a patient presents with either intrinsic or extrinsic staining or discoloration and seems to be a candidate for tooth bleaching, there is a variety of factors and options for the clinician to consider. What is the cause for the discoloration? Is there tooth trauma involved, or has the affected tooth been endodontically treated? What is the best delivery method for the patient’s lifestyle, financial situation, and commitment level to home care? Single dark teeth present a unique challenge for color change and the clinician must be aware of the basic principles of changing the color of one or more teeth in order to implement a successful treatment plan.
The Initial Examination
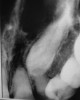
The first and most important consideration is to determine the cause of the tooth discoloration. A clinical examination is conducted, which includes evaluation of the color of the teeth and the adjacent gingiva (Figure 1). Additionally, transillumination, radiographs, and pulp testing may be appropriate. Radiographs should always be taken of a single dark tooth, as teeth can undergo pulpal necrosis without any other symptom than becoming dark (Figure 2). From this examination, the determination is made of whether the tooth is vital or not. A vital tooth may be darker due to trauma and resultant bleeding into the dental tubules without loss of vitality. Vital teeth may also discolor from internal or external resorption, calcific metamorphosis, as well as decay or leaking restorations on the proximal or lingual surfaces. A non-vital tooth may have become darker from the same reasons as a vital tooth, but also have experienced pulpal death. A tooth that has received endodontic treatment may also later darken, especially if there is a poor seal of the endodontic access opening (Figure 3).
Even if a tooth tests as non-vital, it may not require endodontic therapy. If there is no radiographic evidence of pathology and no clinical symptoms, then there is no reason to initiate endodontic therapy based on vitality testing alone. Often single dark teeth are the result of trauma, which should be determined in the dental history. It can take anywhere from 1 to 20 years after the trauma before any pulpal problems develop.
Additional considerations for the single dark tooth are the color of the gingival tissues around the tooth, as well as whether there is any root structure visible due to recession. A smile analysis is used to determine these conditions as well as the movement of the lip during smiling and whether a “gummy smile” exists. The dentin in the root is different from the dentin in the anatomic crown, and does not bleach well if at all, regardless of whether internal or external bleaching is attempted. Also, discolorations of the gingiva may cause a tooth that may be a perfect color match to not be harmonious. Either of these conditions is magnified if the lip exposes much of the root or gingiva because of a hyperactive lip or gummy smile.
Trauma and Calcific Metamorphosis
Many studies suggest that the prevalence of traumatic dental injuries (TDI) is high, although significant variation occurs between countries, populations, age, and gender.1-4 Epidemiological studies, while not always comparable, support the growing body of evidence that TDIs represent a significant challenge for clinicians.5 A study by Koste and colleagues reported that 25% of 6- to 50-year-olds in the United States had experienced a TDI.6 Approximately 30% of children have sustained a TDI to their primary dentition, and 25% of all school-aged children have experienced a TDI.7-9 Other reports document that luxations represent the majority of primary teeth injuries, whereas crown fractures constitute the most commonly occurring injury in permanent teeth.10,11 Also, studies have reported that 71% to 92% of TDIs occur by age 19.12
The etiology of dental injuries varies by age. In the 0 to 6 age group, falls predominate.13 As children enter school, falls, collisions with other children and objects, as well as participation in organized physical activities and sports contribute to dental injuries.9,14-16 TDIs in the teen and young-adult age group are more the result of sports and motor vehicle accidents.14 Several studies have documented that approximately one third of dental injuries are sports-related.15-23 Other causes of TDIs include physical abuse, fights, and assaults—often involving alcohol as an aggravating factor.24-26
The pulp can respond to trauma in a limited number of ways. Primarily it can survive, die, or undergo pulp canal obliteration (PCO), often referred to as calcific metamorphosis.27 The latter represents a common finding subsequent to luxation injuries, 3.8% to 24%, and root fractures, 69% to 73%.2,28-30 The precise mechanism of PCO is not known but disruption of the neurovascular bundle appears to stimulate the rapid formation of hard tissue (dentin or osseous) beginning within the pulp chamber and progressing along the pulp canal walls.31 It may present as partial or total obliteration of the pulp canal space. Although radiographs may reveal what appears to be total obliteration of the pulp canal, generally there remains clinical evidence of a pulp canal and pulpal tissue.32,33 Clinically, the tooth will appear dark yellow due to the increased deposition of underlying dentin. Additionally, there may be a gradual diminution in response to electrical and thermal pulp testing. PCO occurs more frequently in teeth with open apices and in more severe luxation injuries involving displacement.2,34 Extrusive and lateral luxation injuries in immature permanent teeth have demonstrated high rates of PCO.35 A recent study by Netto and colleagues reported the chances of PCO in intruded permanent teeth to be six times greater than in mature teeth, open vs closed apex, and that PCO occurred in 26.7% of such injuries.36 PCO can occur in subluxated and crown-fractured teeth, although with less frequency.37
As mentioned previously, PCO is a common occurrence after root fractures. The location of PCO is thought to be indicative of the type of healing. PCO in the apical segment only is suggestive of hard-tissue callus formation, whereas PCO in the coronal segment or in both coronal and apical fracture segments is indicative of connective tissue repair of the fracture.2,38
Pulp necrosis as evidenced by periapical radiolucency is an infrequent sequela to PCO occurring in approximately 7% to 16% of cases; consequently, prophylactic endodontic therapy is not recommended by most authors.28,39-41 Teeth with PCO likely have diminished healing capacity, and it is not well established whether a secondary trauma or additional dental treatment causes necrosis. In some instances, such as preparing a tooth with PCO for an abutment, it may be prudent to perform prophylactic endodontic therapy before the definitive restorative procedure. A recent article by daCunha and colleagues suggests implementing endodontic therapy prior to development of a periapical radiolucency in a tooth with PCO, based on two major considerations: (1) the technical difficulty and complications that may occur in treating these teeth; and (2) their review of a study that demonstrated a 97.9% success rate for teeth treated without periapical radiolucencies vs a 62.5% success rate for teeth treated with periapical radiolucencies.42 Specific clinical situations will dictate clinical decisions; however, given the relatively low incidence of pulp necrosis in teeth with PCO, endodontic treatment usually is not recommended in the absence of a periapical radiolucency or symptoms. Nonetheless, if a periapical lesion develops, endodontic therapy can be both challenging and fraught with complications (Figure 4). The use of operatory microscopes in the hands of a skilled clinician is warranted and improves the chances of a successful outcome.
Most traumas to primary teeth are luxation injuries that frequently result in radiographic evidence of PCO. Although this may or may not result in crown discoloration, it ceases to be a concern for the patient, parent, or clinician as the tooth is eventually exfoliated. The only indication for bleaching primary teeth, which are generally very light, is trauma that caused the tooth to become dark and the patient is being affected psychologically by the darker teeth. There is no indication for endodontic therapy.
In contrast, younger patients who sustain TDIs where development of the permanent tooth is incomplete, PCO in the form of a discolored incisor presents a long-term esthetic challenge. The most conservative approach to managing PCO-induced discoloration is bleaching without endodontic therapy.
Tray Bleaching
There are a number of types of bleaching techniques to consider for both vital and non-vital teeth, but these types may be divided mainly into those performed in-office or those continued at home. With the advent of nightguard vital bleaching involving tray application of 10% carbamide peroxide, a method for bleaching single dark teeth became more readily available, and did not involve the use of highly caustic chemicals.43 The original recommendation for a single dark tooth was to make a non-scalloped, no-reservoir tray, and bleach all the teeth. The tooth that was darker generally took longer, so an “X” was made on that tooth mold of the tray so the patient could continue to bleach that tooth longer than the other teeth. The use of the “X” on the teeth to be bleached was also helpful when the patient already had crowns on some teeth, and placing bleaching material on them was a waste of material. While this tray system was simple and effective, it did not always result in a perfect match of the teeth. All the teeth would lighten, but often the darker tooth was not able to lighten as much as the normal teeth, and the resultant outcome was lighter teeth, but still with one tooth slightly darker than the others. Some authors have recommended using a reservoir on the darker tooth, but the use of reservoirs has not been shown to increase bleaching efficacy.44 It is not possible to “spot bleach” a tooth either, because the bleaching material goes through the enamel and dentin to the pulp in 5 to 15 minutes, and bleaches under restorations and from one surface to the other (facial to lingual). It has also been shown to bleach beyond the borders of the tray, generally to the cementoenamel junction (CEJ), even if the tooth is only partially erupted.
The ideal bleaching tray is fabricated on a horseshoe-shaped cast with no vestibule to provide good adaptation of the bleaching tray material. Also, the cast should be trimmed such that the central incisors are vertical to avoid folds on the facial. One challenge in fabrication of the single-tooth or regular bleaching tray is trimming the cast without abrading either the teeth or the gingiva. This outcome is accomplished by trimming the cast from the base rather than the sides (Figure 5).
Single-Tooth Bleaching Tray
An improvement on this concept is the use of the “single-tooth” bleaching tray when one tooth is darker, but the other teeth are reasonably acceptable (Figure 6). In this tray design, a conventional non-scalloped, no-reservoir tray is fabricated. Then the teeth molds on either side of the dark tooth are removed (Figure 7 and Figure 8). The patient is given one syringe of bleaching material and applies it only to the single dark tooth mold and sleeps in the appliance. Teeth will bleach at different rates and to different color levels. The goal is to determine how light the single dark tooth will bleach first. If the color of the single dark tooth does not get as light as the surrounding teeth, then the other teeth are not bleached (Figure 9) and the closest match has been achieved. If the single dark tooth matches the other teeth then, again, the other teeth are not bleached. Only if the single dark tooth gets lighter than the adjacent teeth should they be bleached, and in that case, daytime bleaching in short intervals should be used to avoid getting the adjacent teeth lighter than the single dark bleached tooth. Generally, the patient should be informed that the bleaching time for the single dark tooth is about 8 weeks, although it is highly variable.
Endodontically Treated Anterior Teeth
If the dark tooth has already received endodontic therapy, then additional considerations for the discoloration include remaining pulp materials in the pulp chamber, endodontic sealer or filler in the pulp chamber, and dark or leaking restorations in the endodontic access opening, as well as endodontic failure. The type of filler is also important, as silver points require different considerations from gutta-percha fillers. Treatment considerations also may depend on when in the endodontic treatment and subsequent follow-up the tooth was noticed to be dark.
Endodontically treated teeth may be treated from the inside, the outside, or both. The decision for inside or outside depends on a knowledge of what has occurred inside the tooth during the endodontic therapy, as well as the type of restoration used to seal the access opening. The tooth may have received a satisfactory endodontic treatment and been subsequently restored with an acceptable lingual composite that matched the tooth color. However, in subsequent years, the tooth may have discolored (Figure 10). In this situation, the decision for bleaching favors external bleaching, because going inside the tooth to remove the composite will weaken the tooth (Figure 11). However, the choice not to go inside the endodontic tooth depends on whether the treating dentist is aware of the extent to which the pulp chamber was debrided during endodontic therapy, as well as the height in the chamber of the cement and filler.
In-Office Bleaching
In-office bleaching is the oldest form of bleaching. Attempts to bleach single dark teeth date back to the 1800s, and bleaching a single dark tooth was one of the first bleaching research areas.45 A number of materials have been used, but hydrogen peroxide has been the historic favorite. The high concentration of hydrogen peroxide could be applied externally or internally, and often involved heat and light. The classic non-vital in-office bleaching technique involved the placement of 35% hydrogen peroxide into the pulp chamber, and increasing the chemical reaction by the use of heat or light. However, this technique lacks precise control as to the amount of lightening. More critically, when cases of external or internal resorption were evaluated, there were four common concerns listed: 1) teeth had received trauma; 2) high concentrations of peroxide were used; 3) high heat was used to enhance the bleaching, and 4) there was no seal over the gutta-percha. Although the dentist cannot control the trauma, elimination of the other three areas under dental control should be done to lessen the chances of resorption and loss of the tooth. Other possibilities for resorption include the fact that 10% of teeth do not have a connection between the enamel and cementum, with possible percolation of hydrogen peroxide into the surrounding areas, lowering the pH. Using a bleaching product with a higher pH or a salivary catalase are attempts to reduce resorption issues.
Walking Bleach Technique
The change in in-office bleaching led to the next step of “walking bleaching.” In this technique, the gutta-percha was removed 2 mm below the CEJ and a base was applied to seal the endodontic filling material from the pulp chamber. Then, initially, a high concentration of hydrogen peroxide was applied, sealed, and the patient “walked out of the office” while the hydrogen peroxide oxidized the discoloration. This treatment took anywhere from 1 to 6 weekly applications. The challenge was that the high concentration of hydrogen peroxide could be caustic to either the dentist or the patient. Later, this technique evolved into mixing the hydrogen peroxide with sodium perborate to form a mixture that was easier to handle. Sodium perborate breaks down into about a 3% solution of hydrogen peroxide. Finally, the high concentration of hydrogen peroxide was eliminated and sodium perborate alone was used. Internal bleaching treatment was followed by the use of a catalase to neutralize the hydrogen peroxide and elevate the pH around the tooth. With any bleaching treatment, time should be allowed for the shade to stabilize and the oxygen to dissipate from the tooth. If bonding is initiated immediately after bleaching, there is a 25% reduction in bond strengths due to the inhibition of the composite set from the oxygen in the tooth, resulting in shorter enamel tags. It generally takes about 2 weeks or longer for the shade to stabilize and the bond strength to return to normal.
Later, 10% carbamide peroxide was found to be equally as effective as sodium perborate for internal bleaching, at the same concentration, with the additional benefit of causing a rise in pH, which may be beneficial to avoid resorption. A 10% solution of carbamide peroxide is equivalent to 3.5% hydrogen peroxide and 6.5% urea. It is the urea that causes the increase in pH within 5 minutes after application to a level above 8, which cannot be accomplished with hydrogen peroxide alone. Also, the carbamide peroxide has a slower peroxide release and is active longer than hydrogen peroxide. This slower application of peroxide seems to favor the rate of color change. Because trauma is one of the initiators of resorption, that event cannot be totally eliminated. Even teeth that have not been bleached can begin to have resorption, so there is always that possibility. Traumatized teeth should have recall radiographs taken every 1 to 2 years, whether they have been bleached or not.
Inside Bleaching
When performing internal bleaching on a non-vital tooth that has received endodontic therapy, it is important to clean out the inside of the pulp chamber (Figure 12). Often, when endodontic therapy is performed because of trauma, the pulp chamber is large, with high pulp horns. The access opening to the apex may not include debridement of the chamber (Figure 13). The restorative dentist should open the access opening enough to access both the incisal extent as well as the lateral extent of the pulp chamber. Often, removal of the remaining pulp chamber will significantly alter the color of the tooth, even before the bleaching has begun (Figure 14).
Inside-Outside Open Bleaching
In special patients and situations, the dentist may chose to perform inside and outside bleaching while leaving the access opening unrestored. In this situation, the patient injects carbamide peroxide into the pulp chamber and the tray, then seats the tray in the mouth to protect the opening. While this may shorten treatment time due to the continued application of fresh bleaching material, it is essential that the patient be able to perform their part, and also return to the office to have the opening closed. While the tooth will not get any tooth decay during the bleaching process due to the increase in pH afforded by the carbamide peroxide,46 there is the danger that the patient may cease bleaching but not return in a timely fashion to have the orifice sealed. If the office is not equipped to fabricate the additional single-tooth tray, then the standard replacement of the internal carbamide peroxide is performed weekly, taking 1 to 6 office visits for completion. A provisional restoration maintains the seal, and the patient is instructed to call the office immediately if occlusion or food disrupts the provisional seal.
Bleaching or Crown Decisions
The question is often asked why the anterior endodontically treated tooth is not crowned today as it once was in the past. One reason for the resurgence of bleaching single anterior teeth is that the research has shown that while posterior teeth that have received a root canal should be crowned, anterior teeth should only be crowned if they needed a crown regardless of the endodontic therapy. The reason is because the single greatest predictor of survival of an endodontically treated tooth is the amount of remaining dentin. If an intact anterior tooth has a root canal, the external enamel and dentin is still intact. Preparing the tooth for a crown after the endodontic treatment removes the remaining dentin and results in a premature loss of the tooth. Research has also shown that the post does not strengthen the tooth, and cannot compensate for the loss of dentin. Hence, the tooth has a better prognosis to be bleached and restored with composite than to receive a post, core, and crown.
Conclusion
The single dark tooth is an esthetic challenge regardless of the treatment approach. Bleaching the single tooth alone is the safest, most conservative approach to determining the response of the single tooth before changing the adjacent tooth colors. A “single-tooth” bleaching tray is the tray of choice for external bleaching. Single dark teeth with calcific metamorphosis should not be treated endodontically unless there are clinical symptoms of pain or radiographic evidence of an abscess.
For internal bleaching of an endodontically treated tooth, a “walking bleach” approach using 10% carbamide peroxide internally seems to afford the safest approach over previous traditional methods. The combination of one internal bleaching appointment to debride the pulp chamber, followed by tray bleaching with a single-tooth tray or full non-scalloped, no reservoir tray provides the flexibility of unlimited time of treatment without incurring significant in-office charges. Additionally, waiting 2 weeks after bleaching for the shade to stabilize and the bond strengths to return to normal and then using internal composite bonding can harmonize final shade discrepancies. Regardless of the technique used for bleaching, a relapse is possible in 1 to 3 years, and is generally best addressed by outside bleaching in a single-tooth tray with 10% carbamide peroxide to re-bleach the tooth until it matches the surrounding teeth.
References
1. Glendor U, Halling A, Andersson L, Eilert-Petersson E. Incidence of traumatic tooth injuries in the county of Västmauland, Sweden. Swed Dent J. 1996;20:15-28.
2. Andreasen JO, Andreasen FM, Andersson L. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 4th ed. Oxford, England: Blackwell Munskgaard; 2007.
3. Davis GT, Knott SC. Dental trauma in Australia. Aust Dent J. 1984;29:217-221.
4. Brunner F, Krasti G, Filippi A. Dental trauma in adults in Switzerland. Dental Traumatol. 2009;25:181-184.
5. Glendor U. Epidemiology of traumatic dental injuries—a 12 year review of the literature. Dent Traumatol. 2008;24:603-609.
6. Kaste LM, Gift HC, Bhat M, Swango PA. Prevalence of incisor trauma in persons 6-50 years of age: United States, 1988-1991. J Dent Res. 1996;75:696-705.
7. Petti S, Tarsitani G, Arcadi P, et al. The prevalence of anterior tooth trauma in children 6 to 11 years old. Minerva Stomatol. 1996;45:213-218.
8. Rocha MJ, Cardoso M. Traumatized permanent teeth in Brazilian children at the Federal University of Santa Catarina, Brazil. Dent Traumatol. 2001;17:245-249.
9. Flores MT. Traumatic injuries in the primary dentition. Dent Traumatol. 2002;18:287-298.
10. Hedegård B, Stalhane I. A study of traumatized permanent teeth in children aged 7-15 years. Part 1. Swed Dent J. 1973;66:431-450.
11. Gelbier S. Injured anterior teeth in children. A preliminary discussion. Br Dent J. 1967;123:331-335.
12. Davis GT, Knott SC. Dental trauma in Australia. Aust Dent J. 1984;29:217-221.
13. Kramer PF, Zembruski C, Ferreira SH, Feldens CA. Traumatic dental injuries in Brazilian preschool children. Dent Traumatol. 2003;19:299-303.
14. Skaare AB, Jacobsen I. Dental injuries in Norwegians aged 7-18 years. Dent Traumatol. 2003;19:67-71.
15. Hosnik A. Emergency treatment of dentoalveolar trauma. Phys Sports Med. 2004;32(9):1-10.
16. Onetto JE, Flores MT, Garbarino ML. Dental trauma in children and adolescents in Valparaiso, Chile. Endo Dent Traumatol. 1999;10:223-227.
17. Cornwell H. Dental trauma due to sport in the pediatric patient. Calif Dent Assoc J. 2005; 33(6)457-461.
18. Zerman N, Caralleri G. Traumatic injuries to permanent incisors. Endod Dent Traumatol. 1993;9:61-64.
19. Skaare AB, Jacabsen I. Etiological factors related to dental injuries in Norwegians aged 7-18 years. Dent Traumatol. 2003;19:304-8.
20. Gassner R, Bösch R, Tulit, Emskoff R. Prevalence of dental trauma in 6000 patients with facial injuries: Implications for treatment. Oral Surg Oral Med Oral Path Oral Radiol Endod. 1999;87:27-33.
21. Brunner F, Krasti G, Filippi A. Dental trauma in adults in Switzerland. Dent Traumatol. 2009;25:181-184.
22. Promoting oral health: interventions for preventing dental caries, oral and pharyngeal cancers and sports related craniofacial injuries: a report on recommendations of the Task Force on Community Preventive services. MMWR. 2001;50(RR21):1-13.
23. Tuli T, Hachl O, Hohlrieder M, et al. Dentofacial trauma in sports accidents. Gen Dent. 2002;50(3):274-279.
24. Needleman HL. Orofacial trauma in child abuse: types, prevalence, management and the dental profession. Pediatr Dent. 1986;8:71-80.
25. Dimitroulis G, Eyre J. A 7-year review of maxillofacial trauma in a central London hospital. Br Dent J. 1991;170:300-302.
26. Perkeentupa U, Laukkanen P, Veijola J, et al. Increased lifetime prevalence of dental trauma is associated with previous non-dental injuries, mental distress and high alcohol consumption. Dent Traumatol. 2001;17:10-16.
27. Feiglin B. Dental pulp response to traumatic injuries—a retrospective analysis with case reports. Endod Dent Traumatol. 1996;12:1-8.
28. Amir FA, Gutmann JL, Witherspoon DE. Calcific metamorphosis: a challenge in endodontic diagnosis and treatment. Quintessence Int. 2001;32:447-455.
29. Andreasen J. Luxation of permanent teeth due to trauma. Scand J Dent Res. 1970;78:273-286.
30. Andreasen FM, Yu Z, Thomsen BL, Andersen PK. The occurrence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol. 1987;3:103-15.
31. Robertson A, Andreasen FM, Bergenholtz G, et al. Incidence of pulp necrosis subsequent to pulp canal obliteration from trauma to permanent incisors. J Endod. 1996;22:557-606.
32. Kuyk JK, Walton RE. Comparison of the radiographic appearance of root canal size to its actual diameter. J Endod. 1990;16(11):528-533.
33. Piatteli A. Generalized “complete” calcific degeneration or pulp obliteration. Endod Dent Traumatol. 1992;8:259-263.
34. Jacobsen I, Kerekes K. Long term prognosis of traumatized permanent anterior teeth showing calcifying processes in the pulp cavity. Scand J Dent Res. 1977;85(7):588-598.
35. Holcomb JB, Gregory WB Jr. Calcific metamorphosis of the pulp; its incidence and treatment. Oral Surg Oral Med Oral Pathol. 1967;24(6):825-830.
36. Netto JJ, Gondim JO, deCarralho FM, Giro EM. Longitudinal clinical and radiographic evaluations of severely intruded permanent incisors in a pediatric population. Dent Traumatol. 2009;25(5):510-514.
37. Robertson A. A retrospective evaluation of patients with uncomplicated crown fractures and luxation injuries. Endod Dent Traumatol. 1998;14:245-256.
38. Andreasen FM, Andreasen JO, Bayer T. Prognosis of root fractured permanent incisors: prediction of healing modalities. Endod Dent Traumatol. 1989;5:11-22.
39. Schindler WG, Gullickson DC. Rationale for the management of calcific metamorphosis secondary to traumatic injuries. J Endod. 1988;14(8):408-412.
40. Smith JW. Calcific metamorphosis: a treatment dilemma. Oral Surg Oral Med Oral Pathol. 1982;54(4):441-444.
41. Akertblon A, Hasselgren G. The prognosis for endodontic treatment of obliterated root canals. J Endod. 1988;14(11)565-567.
42. daCunho FM, deSouza IM, Monnerat J. Pulp canal obliteration subsequent to trauma: perforation management with M.T.A. followed by canal localization and obturation. Brazilian J Dent Traumatol. 2009;1(2):64-68.
43. Haywood VB. Tooth Whitening: Indications and Outcomes of Nightguard Vital Bleaching. Hanover Park, Ill: Quintessence; 2007.
44. Haywood VB. The “bottom line” on bleaching 2008. Inside Dentistry. 2008;4(2):82-89.
45. Haywood VB. History, safety, and effectiveness of current bleaching techniques and applications of the nightguard vital bleaching technique. Quintessence Int. 1992;23:471-488.
46. Haywood VB. Orthodontic caries control and bleaching. Inside Dentistry. 2010;6(4):36-50.
About the Authors
Van B. Haywood, DMD
Professor
Director of Dental Continuing Education
Department of Oral Rehabilitation
School of Dentistry
Medical College of Georgia
Augusta, Georgia
Anthony J. DiAngelis, DMD, MPH
Chief Department of Dentistry
Hennepin County Medical Center
Minneapolis, Minnesota
Professor
University of Minnesota
Minneapolis, Minnesota