

Sinus Bone Grafting for Dental Implant Placement: A Comprehensive Overview for the General Dentist
Michael Tischler, DDS
It is vital for a general dentist to understand the fundamentals of bone grafting the maxillary sinus. The general dental practice is seeing an increasing group of patients who are living longer, and this group of older baby boomers often has an edentulous posterior maxilla either unilateral or bilateral. When edentulous, the posterior maxilla more likely has diminished bone height, which does not allow for the placement of dental implants without creating additional bone. Through grafting the maxillary sinus, bone of ideal quality can be created (allowing for placement of dental implants), which offer many advantages over other tooth replacement modalities. With the prosthetic aspect of dentistry driving the success of implant dentistry, it is imperative for the general dentist to be aware of the indications, treatment planning, and overall techniques of the sinus bone graft so that patients can be treated or referred correctly.
This article outlines bone grafting of the maxillary sinus for the purpose of placing dental implants. The history, indications, treatment planning, and clinical examples of maxillary sinus grafting are presented as an overview for the general dentist.
SINUS GRAFTING HISTORY AND INDICATIONS
Boyne was one of the first to graft the maxillary sinus for an increase in bulk of osseous tissue in the 1960s.1 At the time, this was actually done to allow for fabrication of a denture when an increase of vertical height was needed. In the late 1960s, Linkow elevated the sinus membrane for the placement of blade implants.2 Tatum created a technique that involved in-fracturing the ridge crest and lifting the sinus membrane and using autogenous bone as the primary graft material in the mid-1970s.3 Tatum in the 1980s furthered the technique using a lateral approach and including synthetic bone. In 1984 Misch organized a systematic approach to sinus grafting based on available bone height and implant design.4 The advances subsequent to the 1980s have allowed sinus grafting today to be a predictable and safe modality with a long-term success rate.5
Once teeth are lost, there will be subsequent bone loss.6 The posterior maxilla bone is less dense than the rest of the mouth, and as teeth are lost, the sinus membrane drops inferiorly, creating less bone for implant placement. The combination of diminished bone and increased posterior bite forces creates a potentially difficult situation for placement of dental implants.7 Through grafting the maxillary sinus, the sinus membrane can be elevated, and bone can be created through a remodeling process that will predictably support tooth replacement by dental implants.8
TREATMENT PLANNING FOR SINUS GRAFTING
Because sinus grafting is a surgical procedure, one of the first areas of treatment planning is to evaluate the patient’s medical history. As well as the standard review of medications, special consideration should be made to patients on bisphosphonates and their relationship to osteonecrosis with oral surgical procedures.9 The author uses a standard sinus graft preoperative pharmacological protocol consisting of: 150 mg of Augmentin BID for 10 days starting the day before surgery (Ceftin can be given if the patient is allergic); Peridex rinse; 800 mg of ibuprofen 1 hour before surgery; Lortab 7.5; and a Medrol dose pack. Any uncontrollable disease should be considered a contraindication to proceeding with a sinus bone graft. Pregnant women should delay having this procedure preformed until after giving birth. Smoking while undergoing a sinus graft should be severely discouraged, yet the literature proves it to be a consideration, not an absolute contraindication.10
Certainly, one of the key parameters to treatment planning any bone graft is to consider the prosthetic end result in relation to the healed graft. Through defining the final prosthetic end position in relation to the opposing arch, it can be determined if ridge height needs to be augmented in conjunction to a sinus graft. The goal is to reduce stress on the dental implants through creating a favorable implant-to-crown ratio.11 Another consideration that relates to graft success is provisionalization during the grafting and the implant healing process. The goal is to eliminate movement on the graft while it is healing so that there is minimal impingement of the graft. This can be obtained through either a fixed provisional or using a denture with a soft reline material and relief at the surgical site. If possible, patients are not to wear a removable prosthesis for 1 week to 2 weeks after surgery to avoid incision line opening.
Radiographic diagnosis can be initially defined through a panoramic x-ray, but it is the author’s opinion that a computerized tomography scan (CT) should be performed before all sinus grafts. The CT will show anatomical abnormalities such as septa, cysts, and oral-antral communications; it will also define patency of the osteomeatal complex (Figure 1). Any abnormal finding on the CT should be referred to an ear, nose, and throat specialist so that the condition can be addressed and clearance for grafting can be obtained. A CT will also define the amount of graft material needed and indicate how much bone is available to support a dental implant.12 A cone beam CT adds the additional benefits of a three-dimensional view with markedly less radiation than a traditional fan beam CT.13
SINUS ANATOMY AND PHYSIOLOGY
The maxillary sinus warms air, lightens the cranium, filters contaminants, and adds resonance to the voice. Interestingly, grafting the sinus has no perceptible effect on changing the tone or pitch of a person’s voice.14
The objective of grafting the maxillary sinus is to lift the sinus membrane superiorly and create adequate bone to support dental implants. Before this can be performed an understanding of the anatomy of the maxillary sinus must be ascertained.
The maxillary sinus is the largest of the four paranasal sinuses with a mean volume in adults of 15 cubic centimeters.15 The shape of the sinus is pyramidal with four boney walls with the apex pointing toward the zygomatic bone (Figure 2 and Figure 3). The superior wall is formed by the thin orbital wall. The posterior wall is related to the pterygomaxillary area of the skull. The medial wall of the sinus is adjacent to the nasal fossa. The lateral wall forms the posterior maxilla. Each of these walls contains vascular structures that must be considered during surgery.7 Arteries supplying the maxillary sinus are mainly from the superior alveolar branches of the maxillary artery. Branches of the descending and greater palatine arteries supply the floor of the sinus. Innervations of the sinus are from the anterior, middle, and posterior superior alveolar nerves.16 As the maxillary alveolar process decreases in volume, there is an associated decrease in vascular vessels.15 The sinus membrane, called the schneiderian membrane, is between 0.13 mm and 0.5 mm thick, and is an immunological barrier.15 The sinus membrane is similar to the membranes in the other paranasal sinuses but has less vascularity creating a pale color. The sinus membrane contains cilia that create a transport system to the ostium for drainage of mucus.7 When performing sinus grafting surgery, it is not uncommon for the sinus membrane to tear upon manipulation.
GRAFTING TECHNIQUES
The amount of bone from the ridge crest to the floor of the sinus can vary, from being several millimeters thick to being eggshell thin. It is the objective of the surgeon to lift the sinus membrane so as to allow enough graft material to allow for placement of adequate sized dental implants. The author uses a sterile protocol for this procedure to reduce exogenous bacteria into the surgical site (Figure 4). An electric handpiece with sterile saline is also used, so that air is not introduced into the surgical site.
The approach to lift the membrane can be achieved from two different directions. If the amount of membrane lift that is needed is between 1 mm to 2 mm, then an osteotome approach can be used from the crest of the ridge. This technique was first developed by Tatum in the mid 1970s. Summers has also contributed toward this concept.17 This is achieved through preparing an osteotomy site 1 mm short of the membrane location then superiorly infracting the membrane with a flat osteotome, lifting the remaining 1 mm of bone and the membrane. This osteotome technique offers great success but is limited to 1 mm to 2 mm of lift. Other methods using a small balloon with saline have been presented in the literature with success as well.18 Up to 8 mm of lift has been reported in the literature with this technique.19
Variations of lifting the sinus membrane from a crestal approach have been presented in the literature. These techniques involve the use of a trephine bur and lifting cores of bone.20
When more than 2 mm of sinus lift is needed, a lateral approach to the membrane is used.21 This offers greater visibility to the sinus and greater surgical con-trol. The lateral wall approach is initiated through accessing the surgical site with a full thickness reflection (Figure 5). A vertical incision mesial to the edentulous area and then a mid-crestal incision on the ridge are performed. Variations of tissue reflection can be made, and is dictated by each anatomical and surgical situation presented.
Once the tissue is reflected, an oval window is prepared into the lateral wall of the maxilla, where the membrane will be lifted (Figure 6). This window is prepared above the crest of the ridge from a lateral aspect, allowing adequate access into the sinus for the placement of graft material and elevation of the membrane. The inferior border of the oval should be 2 mm to 5 mm above the level of the sinus floor. A 6-mm to 8-mm round bur with an electric handpiece can be used or a piezoelectric tip can be used as an alternative.22 The piezoelectric tip offers the advantage of being gentle to the membrane upon contact. This allows for a reduction in damage to the membrane and, therefore, a better containment of graft material. The amount of residual ridge remaining allows for the classification of the sinus type and dictates treatment protocol. The residual oval piece of bone on the wall to be infracted can either be removed from the membrane or left intact (Figure 7). The author chooses to leave the residual bone intact, using it to help elevate the membrane.
According to Misch,7 if there is 12 mm or more of residual ridge remaining, it is classified as an SA-1 site. SA-1 sites allow for placement of a 12-mm implant without manipulation of the sinus membrane. The SA-2 Misch classification allows for osteotomes elevating the membrane when 1 mm to 2 mm of sinus lift is needed. Simultaneous lifting of the membrane and implant placement is done in an SA-2 site. An SA-2 site has 10 mm to 12 mm of vertical residual bone at the crest. An SA-3 Misch classification is when there is at least 5 mm of residual ridge height. With the SA-3 protocol, implant placement can occur at the time of grafting or be delayed 4 to 6 months. This will depend on the quality and quantity of the ridge, and how much initial fixation of the implant occurs. The Misch SA-4 classification occurs when there is less than 5 mm of bone between the crest of the ridge and the maxillary sinus.7 A time period of 6 to 10 months of healing should occur before implant placement. The amount of healing time will be dependent on the amount of autogenous bone in the graft and the healing capacity of the patient.
In a SA-3 or SA-4 sinus lift, the elevation of the membrane should be done carefully to minimize tearing of the sinus membrane. When a membrane is left intact, there is better containment of the graft material. It has been debated in the literature if a tear in the sinus membrane affects the outcome of a sinus graft.23 Various remedies have been presented for repair and classification of the torn membrane.24 When grafting, the author routinely places a collagen membrane on the sinus membrane to act as a barrier of protection so that the graft material does not migrate25 (Figure 8). A resorbable collagen membrane is used for this procedure. A collagen membrane offers many advantages to the surgical site that allow for improved healing.26 These advantages include chemotaxis, fibrinolysis, and hemostasis. A concentrate of the patient’s platelets are used to increase the healing capacity of the site and augment the membrane for containment27 (Figure 9). While many different instruments are available to elevate the sinus membrane from the underlying bone, a piezosurgical tip facilitates elevation.28 It is important to elevate the membrane from all four walls of bone inside the sinus. The medial wall is especially important to elevate so that graft material can have adequate bulk from a buccal?lingual standpoint. Elevation of the membrane off the remaining walls of bone allows for increased blood supply to the graft material (Figure 10). After elevation of the sinus membrane from all four walls of the sinus, the site is ready for delivery of the graft material.
The literature supports various graft materials and combinations of materials.29 A key point is to make sure the graft material is placed into all areas of the sinus where the sinus membrane has been elevated. This ensures that osseous material will be available to support the placement of dental implants after adequate healing. This correct coverage is done through manipulation of the graft material with instruments as it is placed into the sinus (Figure 11). A sterile glass syringe is used to introduce the particulate graft material into the site (Figure 12). The graft material used by the author is a combination of demineralized freeze-dried bone (DFDBA), xenograft, and autogenous bone. A concentrate of the patient’s platelets is used to hydrate the graft combination. The advantages of DFDBA have been substantiated in the literature.30 The osteoinductive nature of DFDBA offers advantages to a graft site.
After placement of the graft material into the sinus, a membrane is placed on the lateral wall to cover the access site (Figure 13). This prevents the infiltration of soft tissue into the grafted site. Some clinicians tack this membrane for improved stability. The author uses a resorbable collagen membrane for this. The final step in a sinus graft is to obtain primary closure of the surgical site. Primary closure helps contain the graft material, and protects the site from exogenous bacteria (Figure 14).
After a sinus graft has healed for the required time, (4 to 8 months) the author routinely takes a post-graft CT to evaluate osseous formation (Figure 15 ; Figure 16 ; Figure 17). This CT indicates the quantity and quality of the graft for implant placement and reinforces the required position of implant placement.31 After implant placement, a final radiograph confirms placement (Figure 18).
CONCLUSION
The sinus graft offers the dental patient a predictable procedure of regenerating lost osseous structure in the posterior maxilla. By following the principles outlined in this article, missing posterior teeth can be restored without the use of a removable prosthesis. This offers the patient many advantages for long-term success. If general dentists understand these concepts, they can better educate their patients and guide them to have the procedure performed.
References
1. Boyne PJ. Lectures to Postgraduate Course. Paper presented at: US Navy Dental School, National Navel Medical Center, 1965-1968; Bethesda, MD.2. Blitzer A, Lawson W, Friedman WH, eds. Surgery of the Paranasal Sinuses, Philadelphia, Pa; WB Saunders: 1985.
3. Tatum OH. Maxillary and sinus implant reconstruction. Dent Clin North Am. 1986;30:207-229.
4. Misch CE. Maxillary sinus augmentation for endosteal implants: organized alternative treatment plans. Int J Oral Implantol. 1987;4(2):49-58.
5. Fugazzotto PA, Vlassis J. Report of 1633 implants in 814 augmented sinus areas in function for up to 180 months. Implant Dent. 2007;16(4): 369-378.
6. Christensen GJ. Ridge preservation: why not? J Am Dent Assoc. 1996;127(5):669-670.
7. Misch CE. Contemporary Implant Dentistry. 2nd ed. St Louis, MO: Mosby Inc; 1999:469-470; 477-484.
8. Tiwana PS, Kushner GM, Haug RH. Maxillary sinus augmentation. Dent Clin North Am. 2006;50(3):409-424.
9. Migliorati CA, Casiglia J, Epstein J, et al. Managing the care of patients with bisphosphonate-associated osteonecrosis: an American Academy of Oral Medicine position paper. J Am Dent Assoc. 2005;136(12):1658-1668. [Published correction in: J Am Dent Assoc. 2006;137(1): 26.]
10. Peleg M, Garg AK, Mazor Z. Healing in smokers versus nonsmokers: survival rates for sinus floor augmentation with simultaneous implant placement. Int J Oral Maxillofac Implants. 2006;21(4):551-559.
11. Misch CE. Consideration of biomechanical stress in treatment with dental implants. Dent Today. 2006;25(5): 80-85.
12. Krennmair G, Krainhöfner M, Maier H, et al. Computerized tomography-assisted calculation of sinus augmentation volume. Int J Oral Maxillofac Implants. 2006;21(6):907-913.
13. Sukovic P. Cone beam computed tomography in craniofacial imaging. Orthod Craniofac Res. 2003;6(Suppl 1):31-6;179-182.
14. Tepper G, Haas R, Schneider B, et al. Effects of sinus lifting on voice quality. A prospective study and risk assessment. Clin Oral Implants Res. 2003;14(6):767-774.
15. Jensen OT. The Sinus Bone Graft. 1st ed. Chicago, Ill. Quintessence Publishing Company; 1999:31-32, 38.
16. Moore KL, Dalley AF. Clinically Oriented Anatomy. 5th ed. Lippincott Williams and Wilkins; 2006:1019.
17. Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15(2):152-162.
18. Soltan M, Smiler DG. Antral membrane balloon elevation. J Oral Implantol. 2005;31(2):85-90.
19. Kfir E, Kfir V, Eliav E, Kaluski E. Minimally invasive antral membrane balloon elevation: report of 36 procedures. J Periodontol. 2007;78(10):2032-2035.
20. Fugazzotto PA. The modified trephine/osteotome sinus augmentation technique: technical considerations and discussion of indications. Implant Dent. 2001;10(4):259-264.
21. Wallace SS, Froum SJ, Cho SC, et al. Sinus augmentation utilizing anorganic bovine bone (Bio-Oss) with absorbable and nonabsorbable membranes placed over the lateral window: histomorphometric and clinical analyses. Int J Periodontics Restorative Dent. 2005;25(6):551-559.
22. Vercellotti T, Pollack AS. A new bone surgery device: sinus grafting and periodontal surgery. Compend Contin Educ Dent. 2006;27(5): 319-325.
23. Wallace SS, Mazor Z, Froum SJ, et al. Schneiderian membrane perforation rate during sinus elevation using piezosurgery: clinical results of 100 consecutive cases. Int J Periodontics Restorative Dent. 2007;27(5):413-419.
24. Vlassis J, Fugazzotto P. A classification system for sinus membrane perforations during augmentation procedures with options for repair. J Periodontol. 1999;70(6): 692-699.
25. Pikos MA. Maxillary sinus membrane repair: report of a technique for large perforations. Implant Dent. 1999;8(1):29-34.
26. Proussaefs P, Lozada J. The use of resorbable collagen membrane in conjunction with autogenous bone graft and inorganic bovine mineral for buccal/labial alveolar ridge augmentation: a pilot study. J Prosthet Dent. 2003;90(6):530-588.
27. Steigmann M, Garg AK. A comparative study of bilateral sinus lifts performed with platelet-rich plasma alone versus alloplastic graft material reconstituted with blood. Implant Dent. 2005;14(3): 261-266.
28. Schlee M, Steigmann M, Bratu E, Garg AK. Piezosurgery: basics and possibilities. Implant Dent. 2006;15(4): 334-340.
29. Scarano A, Degidi M, Iezzi G, et al. Maxillary sinus augmentation with different biomaterials: a comparative histologic and histomorphometric study in man. Implant Dent. 2006;15(2):197-207.
30. Boyan BD, Ranly DM, McMillan J, et al. Osteoinductive ability of human allograft formulations. J Periodontol. 2006;77(9):1555-1563.
31. Tischler M. Interactive computerized tomography for dental implants. Treatment planning from the prosthetic end result. Dent Today. 2004;23(3) 90-93.
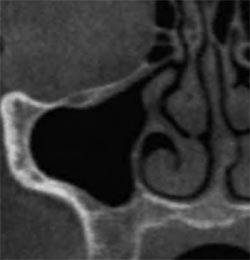 |  | |
| Figure 1 Cross sectional CT view showing patency of the osteomeatal complex. | Figure 2 Three-dimensional CT view showing superior view of the walls of the maxillary sinus. | |
 |  | |
| Figure 3 Skull showing the location of the maxillary sinus. | Figure 4 The author demonstrating the aseptic protocol. | |
 |  | |
| Figure 5 Surgical view of full thickness reflection of the lateral wall of the maxillary sinus. | Figure 6 Oval window preparation of the lateral wall of the maxillary sinus. | |
 |  | |
| Figure 7 Infraction of the maxillary sinus lateral wall. | Figure 8 The collagen membrane being placed in the sinus, below the sinus membrane. | |
 |  | |
| Figure 9 Tubes of the patient's blood were used to concentrate the platelets. | Figure 10 The author ensured that the sinus membrane is lifted off all of the walls of the bone. | |
 |  | |
| Figure 11 Manipulation of the graft material into the sinus. | Figure 12 A sterile glass syringe introduces the graft material into the sinus. | |
 |  | |
| Figure 13 Placement of the collagen membrane on the lateral wall of the sinus. | Figure 14 Primary closure of the surgical site. | |
 | 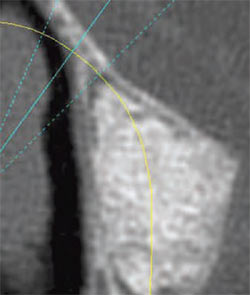 | |
| Figure 15 Cross-sectional view on the CT showing the correct fill of the sinus after healing. | Figure 16 Axial view on the CT showing the correct fill of the sinus after healing. | |
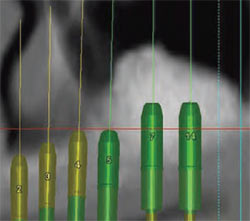 | 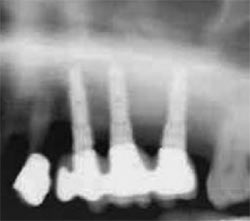 | |
| Figure 17 CT interactive view of the proposed implant placement. | Figure 18 The final radiograph confirms the correct placement into the sinus graft. | |
| About the Author | ||
 Michael Tischler, DDS Michael Tischler, DDS Private Practice Woodstock, New York | ||

