
Integrating Lasers Into a General Practice: My Journey Into Laser Dentistry
Larry Lieberman, DDS
SPRING 2003
In the spring of 2003 I attended the American Academy of Cosmetic Dentistry (AACD) meeting in Orlando, Florida. I attended a seminar by Stewart Rosenberg on the many uses of lasers in dentistry. This proved to be the start of my journey into the exciting field of lasers.
I came away wanting to know more. Although the seminar was very informative I realized there was a bias towards the Biolase laser (Biolase Technology, San Clemente, CA). I have been in dentistry long enough to know that it is always good to get several opinions and then finally come up with the answer that will work for you in your practice. It was time for me to do my “due diligence.” Dr. Rosenberg was promoting the Waterlase® (Biolase Technology). After his seminar it certainly seemed like a good choice. It was promoted for soft and hard tissue; it was a one-wavelength erbium laser that could potentially do it all.
The next morning I met David Hornbrook. After a short conversation with him I decided to look at the Hoya ConBio™ Laser (HOYA Photonics, Fremont, CA) and the Opus Laser (Lumenis, Santa Clara, CA), in addition to the Waterlase. These were the top three erbium lasers.
I came back from the AACD meeting with more questions than answers. I was about to find out that there were many questions to be asked and it was difficult to find out who had the real, unbiased answers. My friend had just gone to an Opus seminar in New York City given by Ken Magid. He came away all excited about the thought of buying a laser just as I had. We proceeded to talk to as many users of the different lasers as we could. Most of the dentists we called were very helpful and seemed to be very honest in their observations and experiences with their different types of lasers. As you could imagine there was a broad range of opinions. Some wouldn’t live without their lasers and some never used them. There is definitely a paradigm shift in philosophy and technique when you embark on the “wonderful world of lasers.”
After speaking with many dentists and sales reps I decided to put a deposit down on the OpusDuo (Erbium [ER:YAG] and CO2 laser) and an Opus 5W (diode). It made sense to get different lasers for hard and soft tissue. I would later realize I really liked having different wavelengths for different types of procedures.
AUGUST 2003
The World Clinical Laser Institute (WCLI) was held in Atlantic City, NJ, in August 2003. The WCLI meeting was quite impressive and quite extravagant. Great music, great food, midnight golf, and lots of lectures on the many uses of the Biolase lasers. There were a lot of Waterlase users present, some prospective buyers, and a few of us that had another laser either ordered or in our office. It was hard to leave that meeting without buying a Waterlase. I was still excited because I was going to be getting delivery of my Opus lasers in a few weeks.
SEPTEMBER 2003
I finally got delivery of my lasers. They were beautiful, smooth, and sexy looking. They had very pretty touch screens and the power to do all those procedures I had read and heard about. Shortly after I got my lasers I went out to San Diego, CA, and worked for a day with Dr. Gerry Weiner. He had a large cosmetic practice, so I felt he could relate to the needs of my practice. It would become very helpful to have somebody with whom I could discuss different procedures. Gerry would become my mentor in laser dentistry. We would talk every 1 to 3 weeks. This really helped getting over the initial learning curve.
THE BEGINNING
When I got back from San Diego I was ready to become a “laser dentist.” I started by doing some of the easier procedures. I would have to learn which laser to use in different situations. The three wavelengths offered a lot of overlap and a lot of differences.
Cavity Preparations
When I wanted to do cavity preparations the erbium laser was my only choice (Table 1). I found that when they say you don’t need anesthetic 85% of the time, it meant that much of the time I would use anesthetic in second molars and the further anterior I would go, the less likely I was to need to get the patient numb. Although I don’t see a lot of children, I’ve found I almost never need to get kids numb for cavity preparations on virgin teeth. The kids love it, the parents love it, and it makes my life a lot easier. After 30 seconds with the laser I may even use a drill without the patient having a negative sensation, as the laser causes an analgesic effect.
The DIAGNOdent (Kavo, Lake Zurich, IL), which is a diode laser (655 nm) that helps in diagnosing decay, and the erbium laser would seem to be a perfect match for any restorative practice that sees children. The DIAGNOdent transmits a light into the tooth and sends back a numerical and audible readout letting the dentist and the patient know that there is decay present with 90% accuracy.1 The DIAGNOdent laser is the least expensive of my lasers (approximately $3,000), and patients really appreciate it.
Soft Tissue
When it came time to do soft tissue work I had several choices. The erbium (Table 2), CO2, and 5W diode laser could all help with soft tissue surgery (Table 3). I found that the CO2 and diode lasers were more effective for bloodless procedures. For my first frenectomy I used a CO2 laser. I used topical anesthetic followed by Citanest® Forte (Dentsply Pharmaceuticals, York, PA). I was delighted to see how easy the frenum disappeared as I lifted the lip with one hand to apply tension and pointed the CO2, laser with the other. To my delight, after 2 minutes the procedure was done both bloodlessly and painlessly. The patient reported no pain after the procedure or at their 1-week postoperative visit. I’ve also done many frenectomies with just topical anesthetic. Emla (AstraZeneca, Wilmington, DE), Tac-Gel (Dental Ventures of America, Corona, CA) and ElaMax™ (Tomi Gion LTD, Alexandria, VA) have all proved effective as topicals. There are many other soft tissue procedures that can be done. I found that the diode laser is best for more detailed and finer procedures as the diode can cut like an electrosurgery unit with many added benefits. A diode will tend to have a smaller zone of necrosis, therefore causing less recession in the cosmetic zone. A big benefit of the diode as well as all lasers is that they can be used judiciously around dental implants.
The CO2 laser is great at vaporizing soft tissue and can be used over large areas such as the lichen planus or in more detailed work such as troughing around crown preparations. The erbium laser will also remove soft tissue with relative ease but hemostasis is much more difficult in most hands (Figure 1; Figure 2View Figure; Figure 3).
Crown Lengthening
When I went to meetings I would try to find a rational approach to doing crown lengthening. Some would say closed flap procedures were always the way to go and some would say that you should always open the flap. I found that the answer for me was somewhere in the middle. I think that closed flap is often times effective on anterior smile line cases. I’ll probe the tissue, mark it, cut it with a diode where I want it to end up, and use my erbium to scallop the bone to create a sulcus similar to what was present before, all the while following the principles of biologic width as described by Orban, Kois, and others.2,3 This has been a tremendous advantage that both myself and the patients love because of the ease of healing and minimal, if any, discomfort. I think there are many times that traditional crown lengthening procedures are definitely indicated and can be more effective, especially when there is a lot of interproximal ramping that is needed. In cases of passive eruption, where the sulcus is deep and the teeth appear short, it is relatively easy to trim the tissue with a diode. These cases may need only soft tissue work and usually heal very quickly. They look good within 1 week and really good after 2 weeks (Figure 4; Figure 5; Figure 6; Figure 7; Figure 8; Figure 9).
OCTOBER 2003
Opus provided a 2-day staff training in Orlando, FL. The training was meant for the dentist but I took several of my key clinical staff. I feel it is important to have the staff knowledgeable about all the procedures we do. When we go to implement something new, it becomes even more important to have everybody on board and supportive. Your staff can have a tremendous effect on the patients’ perception and their acceptance.
APRIL 2004
I attended the Academy of Laser Dentistry (ALD) meeting in Palm Springs, CA. The ALD meeting is not sponsored by any laser company. I was happy to see that it seemed to be without bias. All different types of lasers were represented and they truly tried to present good research. Even at this meeting I could see that using lasers in dentistry was still in its infancy. There were many people looking for answers just as I was.
While I was at that meeting I was introduced to low-level lasers and Millennium Periolase. They would soon be the fifth and sixth lasers in my office.
Low-level laser therapy has been used for more than 30 years but needs more research in this country. It has been shown to be effective in all sorts of inflammatory conditions. I originally bought this diode laser to help my wife. She had torn cartilage in her wrist with a lot of pain. The hand surgeon gave her no guarantee with surgery. Jan Tuner,4 a Swedish dentist, told me that it should help and that I could return it in a month if it didn’t do her any good. He explained that it would decrease the pain by enhancing the synthesis of endorphins, increasing circulation, and decreasing bradykinins and c-fiber activity.5
So far, more than 2 years have passed and my wife has still avoided surgery and the pain seems to be handled effectively with periodic low-level laser therapy (LLLT). There are many other uses of LLLT. It can help headaches, muscle pain, inflammation, and toothaches. If the tooth doesn’t need root canal therapy it can decrease or eliminate the symptoms of an inflamed pulp (Figure 10).
MAY 2005
Periodontal Therapy—Laser Number 6
Lasers have been shown to be effective in periodontal therapy for many years. Soft tissue lasers such as the diode (800 nm to 830 nm, 980 nm) and Nd:YAG (1064 nm) will reduce bacteria and help coagulation during nonsurgical periodontal therapy.6 Both of these wavelengths are well absorbed by melanin and hemoglobin. In most states hygienists can use soft tissue lasers as an adjunct to periodontal therapy.
In May 2005 I saw Ray Yukna, DMD, and Bob Gregg, DDS, give a very convincing presentation for a laser-assisted new attachment procedure (LANAP). Professor Yukna, coordinator of postgraduate periodontics at Louisiana State University, helped get Food and Drug Administration clearance following 3 years of research for the LANAP protocol. The procedure uses the PerioLase® (Nd:YAG) by Millennium Dental Technologies, Inc (Cerritos, CA) to offer a less traumatic alternative to traditional periodontal surgery. The procedure has been shown to be regenerative as opposed to being resective in the elimination of pockets.7 Over the past 2 years I’ve seen consistently good results. I’ve been very excited to see teeth saved that I previously would have thought were hopeless. The Periolase laser is a versatile soft tissue laser that can be used for all soft tissue procedures. Its biggest claim to fame is that LANAP promotes a cementum-mediated new attachment and periodontal regeneration.7 Some people use the analogy that the Periolase may do for gums what Lasix has done for eyes. We can only hope so (Figure 11).
CONCLUSION
When you decide to invest your time and money into lasers do your homework. You need to ask lots of questions so you can be realistic about your expectations. Remember, like anything else there is always a learning curve. Lasers are something new that offer you and your patients many wonderful benefits. Get a mentor. Find a dentist that you can ask questions. It has always helped me to bounce questions off other laser dentists. This was especially helpful for the first several months, and continues to be an invaluable way to get more comfortable doing laser procedures.
The last several years have been an exciting journey. I’m constantly learning and growing in my knowledge of laser dentistry. I’ve met some brilliant and interesting people that I think will help change the way we look at all of medicine and dentistry. I think we’ve just seen the tip of what lasers can really do.
References
1. Attrill DC, Ashley PF. Occlusal caries dectection in primary teeth: a comparison of DIAGNOdent with conventional methods. Br Dental J. 2001;190(8):440-443.2. Gargiulo AW, Wentz FM, Orban B. Dimensions of the dentegingival junction in humans. J Periodontol. 1961:32:261-267.
3. Kois JC. New paradigms for anterior tooth preparation. Rationale and technique. Compend Contin Educ Dent. 1998;88(4):19-30.
4. Tuner J, Hode L. The mechanisms, laser therapy clinical practice and scientific background. Sweden: Prima Book AM. 2002;334-362.
5. Honmura A, Yanase M, Obata J, et al. Therapeutic effect of Ga-AI-As diode laser irradiation on experimentally induced inflammation in rats. Lasers Surg Med. 1992;12(4):441-449.
6. Kreisler M, Meyer C, Stender E, et al. Effect of diode laser irradiation on attachment rate of periodontal ligament cells: an in vitro study. J Periodontol. 2002;72(10):1312-1317.
7. Yukna RA, Evans GH, Rastardis S, et al. Human periodontal regeneration following LANAP. International Association Dental Res. 2004;Abstract #2411.
 |  | |
| Figure 1 Retracted view of 6-year-old boy with obstructive frenum. | Figure 2 Frenectomy healing after 3 weeks. | |
 |  | |
| Figure 3 This tissue has healed and is ready for the needed gingival symmetry. | Figure 4 This patient's central incisors had a crown length of 6 mm. | |
 |  | |
| Figure 5 Preoperative retracted smile view. | Figure 6 Marking the tissue with the diode. | |
 |  | |
| Figure 7 Creating biologic width with the ER:YAG and recreating sulcus depth. | Figure 8 The 6-mm central incisors become 9 mm in crown length. | |
 |  | |
| Figure 9 At the 3-month postoperative point, the centrals are 8.5 mm in length. | Figure 10 Low-level laser therapy (LLLT) unit. | |
 | ||
| Figure 11 (Left to right) Periolase (Nd:YAG), Opus Duo (ER:YAG and CO2), Opus 5W Diode, and the KaVo DIAGNOdent. | ||
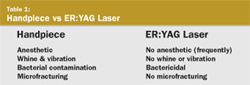 Table 1 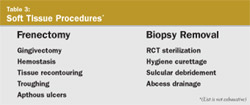 Table 3 | 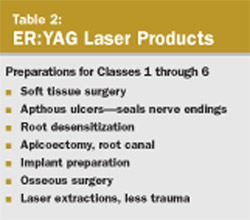 Table 2 | |
| About the Author | ||
 Larry Lieberman, DDS Larry Lieberman, DDSPrivate Practice Palm Harbor, Florida | ||


{kind=link}