

Forced Eruption in the Esthetic Zone as an Option to Implants in the High Lip Line Patient: A Case Report
Robert A. Levine, DDS, and Don G. Katz, DDS, MAGD
The use of dental implants to solve the dilemma of a nonrestorable maxillary anterior tooth has become part of daily treatment planning discussions. The benefits to this procedure include the conservation of adjacent tooth structure by avoiding tooth preparation of the abutment teeth and the improved ability to perform daily plaque control. The replacement of the tooth with a similar permanent prosthesis, which avoids the use of a removable appliance to replace a single tooth, is a notable benefit as well.1-4
Because each patient presents different needs and potential esthetic limitations, a comprehensive exam must be performed when determining the use of a dental implant in the esthetic zone.5-12 The clinical evaluation should include:
- Lip line esthetics (location of the smile line: high, medium/average, low)
- Gingival morphotype (thin with high scallop vs thick with shallow scallop)
- Interocclusal relationship (horizontal and vertical overlap)
- Status of the adjacent dentition (crown integrity, endodontic, and periodontal status)
- Status of the adjacent soft tissue (excessive gingival display/gummy smile or inadequate soft tissue because of gingival attachment loss resulting in gingival recession, gingival asymmetry, or a mucogingival problem)
- Radiographic status (position and axis of adjacent roots, radiolucencies in the alveolar process, vertical bone height), root length of the evaluated tooth, and clinical assessment of the level of the root fracture or resorptive lesion.
This information is helpful in determining the possibility of orthodontic extrusion/forced eruption.
Soft Tissue Determinants
The soft tissue biotype, soft tissue marginal location, tooth form, and interproximal height of bone can help the clinician to determine the appropriate treatment plan.13-16 Evaluation of the two basic tooth forms frequently reflects the type of soft tissue profile and includes:
1. A square tooth form with apically located proximal contacts (beyond one half of the tooth) and a thick, flat gingival biotype are ideal case types for a dental implant. The interproximal bone height, as measured on the adjacent tooth surfaces, is an important key in making the presurgical determination of postoperative gingival recession and soft tissue papillary loss. Interproximal probing depths of 3 mm to 4 mm on adjacent teeth (on bone sounding) confirm a thick gingival biotype. Based on the patient’s clinical presentation, immediate restoration (provisionalization) or customizable healing abutments at surgery to help create the desired emergence profiles by supporting the interproximal papillae during the healing phase are recommended.17,18
2. The triangular tooth form has a more coronally located contact and is usually associated with a thin, scalloped gingival biotype. These case types have the potential to be the most challenging to achieve an esthetic marginal gingival result after implant surgery. This concern would be most noticeable in a high lip line individual. Thus, an alternative plan of a three-unit fixed bridge with extraction/socket preservation along with bone and/or soft tissue augmentation to create an ovate pontic may result in a more pleasing esthetic outcome for this patient. At least 1 mm to 2 mm of soft tissue recession can be anticipated upon extraction when an implant is not placed immediately; therefore, if the soft tissue level presurgically is more apical ( 1 mm to 2 mm) than the contralateral or adjacent tooth,15 additional recession and potential esthetic problems can be expected. Anticipation of any postsurgical recession needs to be discussed with patients before treatment. A more coronally placed presurgical soft tissue profile (1 mm to 2 mm) enables the periodontist to obtain more favorable results postsurgically because normal anticipated recession (1 mm to 2 mm) can result in symmetry of the gingival margins by virtue of this biologic recession.
Because of the predictable recession postsurgery, the patient who has a thin, scalloped gingival biotype and a high lip line becomes the greatest esthetic challenge when faced with a nonrestorable tooth in the esthetic zone. If the patient decides to undergo implant therapy, an understanding of these potential problems needs to be addressed. In addition, the patient needs to be prepared for treatment to modify the site before either orthodontic extrusion with extraction or soft tissue or bone reconstructive surgery for site preparation.19-22
Forced eruption has been successful in the management of nonrestorable teeth in nonesthetic and esthetic areas for the past 30 years when treating fractured teeth.23-30 The benefits of forced eruption include:
1. Preserving adjacent tooth structure by treating the single tooth and avoiding a three-unit bridge or the placement of a single implant which may be contraindicated (for reasons outlined above).
2. Conserving the adjacent hard and soft tissues which is extremely important in the esthetic zone in a high or medium/average lip line individual. Forced eruption avoids the use of conventional osseous crown lengthening, which requires the blending of the tissues (osseous and gingival) and the creation of adequate room for the biologic width.31-37 Thus, a one-tooth problem becomes a threetooth surgical procedure, which creates noticeable tissue recession and asymmetry in the three-tooth surgical crown lengthening scenario.23,27,29
A treatment planning dilemma of the benefits for either procedure can frequently occur in discussion with patients when the esthetic zone is involved. The following case report will examine the benefits and limitations when using forced eruption in a case of a traumatically fractured maxillary central incisor. Furthermore, this case report will expound on the process by which the patient was informed and prepared for a possible change in treatment planning based on continual reassessment of her case by the treating periodontist and restorative dentist during active therapy. Moreover, this case emphasizes the importance of the team approach to her care.
Case Presentation
The Art and Science of Treatment Planning a Complex Esthetic Problem
A 34-year-old woman presented to the restorative dentist on emergency after a traumatic incidence, which resulted in the fracture of tooth No. 8 (Figure 1; Figure 2; Figure 3). Immediate root canal therapy was commenced on both teeth Nos. 7 and 8 as endodontic symptoms were apparent for both teeth, and it was the patient’s desire to try to save both teeth if possible. An electrosurgical unit was used along with a hemostatic agent to create a dry field so that a post and core could be placed (Figure 4 and Figure 5). An acrylic temporary was cemented and the patient proceeded to the periodontist’s office the same day for evaluation of these teeth and treatment planning discussions (Figure 6).
The clinical examination at the periodontist’s office revealed a healthy periodontium with no active periodontal disease. A thin, scalloped gingival biotype was noted with a diastema between teeth Nos. 8 and 9. Clinical and radiographic examination revealed a subgingival root fracture on the palatal aspect of tooth No. 8 to the level of the osseous crest. A root proximity was noted between teeth Nos. 7 and 8, which would make implant placement to replace one or both teeth a potential esthetic problem because of limited space availability.5 The root length of tooth No. 8 was deemed adequate for forced eruption even with the anticipated 5 mm to 7 mm of eruption. The prognosis of both teeth Nos. 7 and 8 were deemed guarded and the following treatment options and concerns were reviewed with the patient:
1. Extraction of tooth No. 8 with socket preservation (bone grafting/guided bone regeneration to preserve the hard and soft tissues) with delayed implant placement or immediate implant placement based on the periodontist’s intrasurgical assessment. Future extraction and immediate implant/socket preservation could not be ruled out for tooth No. 7 as well if symptomatic problems continued for this tooth. A vertical root fracture could not be ruled out for either tooth since the patient was in such a state of discomfort at presentation. With the experience of adjacent implants in the esthetic zone38 and anticipated lack of interproximal papillae formation between the final implant restorations, a discussion of future replacement of the final crown of tooth No. 8 with a cantilever bridge and an ovate pontic to replace tooth No. 7 would be the best esthetic result if tooth No. 7 was lost in the future.
2. A three- to four-unit fixed bridge (teeth Nos. 6 through 9 or 7 through 9 with the extraction of tooth No. 8). The prognosis of tooth No. 7 could not be formulated presently and a provisional would be recommended for 3 months to reevaluate this tooth’s overall healing and its ability to function as an abutment or the need to incorporate tooth No. 6 in the final restoration. The soft tissues would require reevaluation at 3 months for soft/hard tissue reconstruction before the final restoration based on the amount of postextraction recession seen with the extraction defect associated with tooth No. 8.
3. Forced eruption (orthodontic extrusion) by the periodontist to be completed over three to six visits spread out over weekly intervals until clinical, radiographic, and patient symptoms could be better evaluated. If the fracture line could not be fully exposed after completion of forced eruption and flap entry, then continued eruption until extraction (orthodontic extraction) would follow with immediate implant placement.19 This approach would further extrude both the hard and soft tissues coronally, which would allow the periodontist more leeway to provide an esthetic final result. The surgical adjustment of both the hard and soft tissues would then become a “subtraction” procedure (ostectomy/gingivectomy), which is clinically more predictable than an “addition” procedure (hard tissue and/or soft tissue reconstruction). Thus, the periodontist would be able to sculpt the tissues at the surgical implant placement visit to create gingival symmetry. It is the authors’ clinical experience to avoid cases in which previous apical endodontic surgery was performed because the buccal plate fenestration and/or dehiscence will be present at the time of extraction resulting in a needed guided bone regeneration procedure anyway.
Treatment Decision
The patient wanted to do what was necessary to try to save both teeth, and with her complete understanding of the guarded prognosis of them, forced eruption was commenced. The goal was to evaluate whether the subgingival fracture could be brought far enough supragingivally to allow adequate room for the biologic width and a crown margin while still having an adequate root length remaining. If not, orthodontic extraction and an immediate implant would result. Restorative discussions included a patient-desired smile makeover from teeth Nos. 6 to 11 with porcelain veneers anticipated for teeth Nos. 6, 7, 9, 10, and 11. Tooth No. 8 was treatment planned for a porcelain crown. This gave the restorative dentist the ability to adjust the contact points and widths based on the final soft tissue interproximal heights in their corresponding embrasure spaces adjacent to tooth No. 8. This would help to avoid posttreatment black triangles.
The tooth was provisionalized the same day with the restorative dentist and cemented with permanent cement in anticipation of orthodontic forced eruption therapy. Because of inadequate tooth structure lingually, the preparation was intentionally extended into the biologic width to the level of the osseous crest to gain retention.
Forced Eruption Therapy
Orthodontic brackets were bonded to the two teeth on either side of tooth No. 8 to allow the passive fit of a 0.012 round flexible nickel titanium wire. Next, the No. 8 bracket was placed in position approximately 2 mm apical to the level of the wire (Figure 7). The bracket was engaged and orthodontic therapy was commenced followed by incisal reduction of tooth No. 8 out of all excursive movements (approximately 2 mm). Weekly visits were scheduled until adequate tooth structure was created radiographically (ie, for the biologic width and crown margin). In a thin periodontium, 3 mm to 4 mm of sound tooth structure beyond the fracture line is needed. In a thick periodontium, at least 4 mm is needed. It took four visits to erupt the tooth with the periodontist judging when to surgically flap the area and perform soft and hard tissue correction around the tooth (Figure 8; Figure 9; Figure 10; Figure 11; Figure 12). After approximately 5 mm to 6 mm of eruption, a three-tooth, full-thickness flap was elevated (sulcular incisions for teeth Nos. 7 and 9; submarginal incisions for tooth No. 8 buccal/lingual). The tissues associated with tooth No. 8 alone were adjusted without any root instrumentation of the adjacent root surfaces to avoid postsurgical attachment loss with subsequent loss of papillary dimension (Figure 13 and Figure 14).
The major advantage of forced eruption is the maintenance of esthetics and symmetry of contralateral gingival margins by converting a three-tooth osseous crown lengthening procedure to a one-tooth osseous procedure. The final decision to restore the tooth or to continue eruption until extraction with immediate implant placement was made by the restorative dentist. Because he felt that the tooth was presently restorable, he reprovisionalized (Figure 15 and Figure 16) and it was stabilized passively with a larger diameter wire (0.018 round nickel titanium) for retention by the periodontist while tooth No. 10 was derotated for a favorable final prosthetic-esthetic result. Common tying of teeth Nos. 6, 7, and 8 with 0.010 dead soft wire was then done for anchorage followed by stripping of the contact between teeth Nos. 8 and 9. A chain elastic was used to orthodontically move tooth No. 9 mesially to provide additional prosthetic room to bring tooth No. 10 back into a more ideal arch position (Figure 17 and Figure 18). This was completed in three additional visits. Upon completion of derotating tooth No. 10, fiber resection was completed to avoid relapse of this tooth. Three months of healing was recommended after orthodontic eruption of tooth No. 8. The derotation of tooth No. 10 took place during this time frame. The decision was made to go ahead with the final crown on tooth No. 8 because tooth No. 7 had been asymptomatic for months. The esthetic makeover of the maxillary anterior sextant and diastema space closure was then commenced with the patient again being informed of the continued guarded prognosis of both teeth long-term.
Finalization of the Restorative Therapy Treatment Plan
From the time of the initial accident to the final stages of restorative therapy, patients often experience heightened emotions. Traumatic accidents can leave patients unprepared for the treatment decisions they need to make. This patient was happy with the esthetics of her teeth before the accident and never considered the shapes, sizes, color, or position of her teeth. After following the long path from extrusion to surgical correction and postsurgical healing of the tissues, this patient had a difficult time deciding if she wanted her previous diastama between teeth Nos. 8 and 9 closed. Dentists often feel compromised when they are not able to create smiles that are perfect from their prospective. It is important that we provide patients the smiles that they want. Careful dialogue, wax-ups, esthetic imaging, and realistic temporaries help to show our patients the end result.39,40 The patient finally decided on space closure between teeth Nos. 8 and 9 and slight rotation of tooth No. 10 (like her presentation smile). She wanted a minimal rotation of tooth No. 10 with small irregularities in her teeth. Meeting the patient’s esthetic expectations is paramount for a successful case.
Restorative Therapy Sequence
Teeth Nos. 6, 7, 9 through 11 were prepared for porcelain veneers (Figure 19) using a 0.5-mm-depth cutting bur. A soft chamfer was created at the tissue margin and the line angles were followed through the embrasures to create ideal proportions. Tooth No. 8 was prepared for a full-coverage porcelain crown. A full-arch impression was taken with Splash! Putty and light viscosity wash (Discus Dental, Culver City, CA). A face-bow registration was recorded (Stratos 200, Ivoclar NA, Amherst, NY) along with a stick bite registration. This was sent to the laboratory for fabrication of feldspathic veneers for teeth Nos. 6, 7, 9, 10, 11, and crown No. 8. Feldspathic porcelain (Creation, Jensen Industries, Inc, North Haven, CT) was used for its ability to build color into the restoration with less tooth reduction.41 By leaving as much enamel as possible, the tooth is more rigid and there is more foundation to achieve a stronger bond.42 This results are less flexural stress in the restoration, greater bond strength to enamel, and less potential for sensitivity. The provisional veneers and crowns were fabricated with a bis-acryl material (Protemp™ Garant™, 3M™ESPE™, St. Paul, MN). An impression of the wax-up was used and the material was allowed to set directly to the teeth. All flash from the margins was trimmed and polished.
At the cementation stage, the temporaries were sectioned and removed. The teeth were cleaned with a pumice-water slurry in a rubber cup. The restorations were tried in individually to check marginal integrity and then together for evaluation of interproximal contacts. The restorations were then reinserted with RelyX™ try-in paste (3M™ESPE™) to check color and to gain patient approval. A split dam technique was used for isolation during the technique-sensitive process of inserting the restorations. The restorations were re-etched and salinated. The teeth were etched three at a time using 37% phosphoric acid and rinsed well. Gluma® desensitizer (Heraeus Kulzer, Armonk, NY) was applied for 30 seconds followed by OptiBond® F (Kerr Dental, Orange, CA) for 20 seconds and air-dried. All of the restorations were then seated together with RelyX™ (3M™ ESPE™) translucent resin cement. The restorations were held in place and the excess cement was removed from the buccal aspect. A 2-mm Demitron Optilux™ (Kerr Dental) tacking tip was used for 5 seconds on each restoration to hold them in position. The cement on each tooth was then meticulously removed. All of the restorations were cured with a high intensity PAC light (Air Techniques, Melville, NY) for 1 minute. Clean up of the excess cement was then completed with diamond finishing burs and rubber tips and cups (Figure 20 and Figure 21). A Hawley retainer was fabricated and worn at night to stabilize the tooth position postorthodontics (Figure 22; Figure 23; Figure 24).
Discussion
The decision to save a nonrestorable tooth with tooth fracture in the esthetic zone needs to be addressed with special attention to smile line dimension, adequate root length remaining in the bone upon completion of therapy (crown-to-root assessment), gingival biotype, and especially the patient’s desire for self-preservation. The patient’s full understanding of the treatment options, limitations, and long-term prognosis in a proposed treatment plan needs to be fully reviewed frequently on multiple appointments to reinforce this understanding between all of the parties involved.43 In our age of highly successful osseointegration, this final result does not always translate into a successful esthetic clinical result. The issues of postsurgical soft and hard tissue recession, especially in the esthetic-conscious high lip line individual, can mean a failure if their expectations are not met. The team approach to care enables the patient to benefit from each clinician’s professional experiences with regard to that particular problem. As a result, the patient will ultimately benefit.44
ACKNOWLEDGEMENT
The authors would like to thank Natalie Faynburd with Edward Dental Studio in Southampton, PA, for the porcelain work, and Ms. Bari Levine for her editing skills in review of this manuscript.
References
1. Buser D, Weber HP, Bragger U, et al. Tissue integration of one-stage ITI implants: 3-year results of a longitudinal study with hollow-cylinder and hollow-screw implants. Int J Oral Maxillofac Implants. 1991;6(4): 405-412.2. Buser D, Mericske-Stern R, Bernars JP, et al. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a propective multi-center study with 2359 implants. Clin Oral Implants Res. 1997;8(3):161-172.
3. Laney WR, Jemt T, Harris D, et al. Osseointegrated implants for single-tooth replacement: progress report from a multicenter prospective study after 3 years. Int J Oral Maxillofac Implants. 1994;9(1):49-54.
4. Levine RA, Clem DS 3rd, Wilson TG Jr, et al. Multicenter retrospective analysis of the ITI implant system used for single-tooth replacements. Results of loading for 2 or more years. Int J Oral Maxillofac Implants. 1999;14(4):516-520.
5. Buser, D, Martin W, Belser UR. Optimizing esthetics for implant restorations in the anterior maxillae. Anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004;19(suppl): 43-61.
6. Spear FM, Kokich VG, Mathews D. Interdisciplinary management of anterior dental esthetics. J Am Dent Assoc. 2006;137(2): 160-169.
7. Garber DA, Salama MA. The aesthetic smile. diagnosis and treatment. Periodontol 2000. 1996;11:18-28.
8. Levine RA, Randel H. Multidisciplinary approach to solving cosmetic dilemmas in the esthetic zone. Contemporary Esthetics and Restorative Practice. 2001;5(6):62-67.
9. Terry DA, McGuire M. The perio-aesthetic-restorative approach for anterior reconstruction-Part I: Evaluation and periodontal surgery. Prac Proced Aesthet Dent. 2002;14(5): 283-294.
10. Levine RA, McGuire M. The diagnosis and treatment of the gummy smile. Compend Contin Educ Dent. 1997;18(8):757-766.
11. Sonick M. Esthetic crown lengthening for maxillary anterior teeth. Compend Contin Educ Dent. 1997;18(8):807-819.
12. Levine RA, Katz D. Developing a team approach to complex aestetics: treatment considerations. Pract Proced Aesthet Dent. 2003;15(4):301-306.
13. Kois JC. The restorative-periodontal interface: biological parameters. Periodontol 2000. 1996;11:29-38.
14. Kois JC. Altering gingival levels: The restorative connection. Part 1: Biologic variables. J Esthetic Dent. 1994;6(1):3-9.
15. Kois JC. Predictable single tooth peri-implant esthetics: five diagnotic keys. Compend Contin Educ Dent. 2001;22(3):199-206.
16. Salama H, Salama M, Garber D, et al. The interproximal height of bone: a guidepost to predictable aesthetic strategies and soft tissue contours in anterior tooth replacement. Pract Periododont Aesthet Dent. 1998;10(9): 1131-1141.
17. Touati B, Guez G, Saadoun A. Aesthetic soft tissue integration and optimized emergence profile: Provisionalization and customized impression coping. Pract Periodontics Aesthet Dent. 1999;11(3):305-314.
18. Kan JY, Rungcharassaeng K. Immediate placement and provisionalization of maxillary anterior single implants: a surgical and prosthodontic reationale. Pract Periodontics Aesthet Dent. 2000;12(9):817-824.
19. Salama, H, Salama M. The role of orthodontic extrusive remodeling in the enhancement of soft and hard tissue profiles prior to implant placement: a systematic approach to the management of extraction site defects. Int J Periodontics Restorative Dent. 1993;13(4): 312-333.
20. Seibert JS, Salama H. Alveolar ridge preservation and reconstruction. Periodontol 2000. 1996;11:69-84.
21. Buser D, Dula K, Belser U, et al. Localized ridge augmentation using guided bone regeneration. 1. Surgical procedure in the maxilla. Int J Perodontics Restorative Dent. 1993;13(1):29-45.
22. Levine RA, Makrauer Z. Enhancing a cosmetic implant result with periodontal plastic surgery. Contemp Esthet Restorative Pract. 1998;2(4):32-40.
23. Ingber JS. Forced eruption: part II: A method of treating nonrestorable teeth—periodontal and restorative considerations. J Periodontol. 1976;47(4):203-216.
24. Ivey DW, Calhorn RL, Kemp WB, et al. Orthodontic extrusion: its use in restorative dentistry. J Prosthet Dent. 1980;43(4): 401-407.
25. Ross S, Dorfman HS, Palcanis KG. Orthodontic extrusion: a multidisciplinary treatment approach. J Am Dent Assoc. 1981;102(2): 189-191.
26. Pontoriero R, Celenza F Jr, Ricci G, et al. Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. Int J Periodontics Restorative Dent. 1987;7(5):30-43.
27. Levine RA. Forced Eruption, Part II: Esthetic treatment of nonrestorable teeth. Compend Contin Educ Dent. 1988;9(2): 136-140.
28. Rosen PS, Marks MH, Lepine EJ. Comprehensive treatment for a subcrestral fractured incisor in the mixed dentition. Compend Contin Educ Dent. 1991;12(6): 382-387.
29. Levine RA. Forced Eruption in the Esthetic Zone. Compend Contin Educ Dent. 1997;18(8): 795-803.
30. Stevens BH, Levine RA. Forced eruption: a multidisciplinary approach for form, function and biologic predictability. Compend Contin Educ Dent. 1998;19(10): 994-998.
31. Ingber JS, Rose LF, Coslet JG. The “biologic width”—a concept in periodontics and restorative dentistry. Alpha Omegan. 1977;70(3):62-65.
32. Maynard JG Jr, Wilson RD. Physiologic dimensions of the periodontium significant to the restorative dentist. J Periodontol. 1979;50(4):170-174.
33. Nevins M, Skurow HM: The intracrevicular restorative margin, the biologic width, and the maintenance of the gingival margin. Int J Periodontics Restorative Dent. 1984;4(3):30-49.
34. Wagenberg BD, Eskow RN, Langer B. Exposing adequate tooth structure for restorative dentistry. Int J Periodontics Restorative Dent. 1989;9(5):322-331.
35. Becker W, Ochsenbein C, Becker BE. Crown lengthening: the periodontal-restorative connection. Compend Contin Educ Dent. 1998;19(3): 239-256.
36. Wagenberg BD. Surgical tooth lengthening: biologic variables and esthetic concerns. J Esthet Dent. 1998;10(1):30-36.
37. Pontoriero R, Carnevale G. Surgical crown lengthening: a 12-month clinical wound healing study. J Periodontol. 2001;72(7): 841-848.
38. Tarnow DP, Cho SC, Wallace SS. The effect of inter-implant distance on the height of inter-implant bone crest. J Periodontol. 2000;71(4):546-549.
39. Gurel G, Bichacho N. Permanent diagnostic provisional restorations for predictable results when redesigning the smile. Pract Proced Asthet Dent. 2006;18(5):281-286.
40. Brooks L. The many uses of cosmetic imaging. Dent Today. 2006:25(6): 106-108.
41. Spear F. Treatment planning, tooth reduction and margin placement for anterior indirect esthetic restorations. Advanced Esthetics and Interdisciplinary Dentistry. 2005;1(4):4-13.
42. Magne P, Douglas WH. Porcelain veneers: dentin bonding optimization and biometric recovery in the crown. Int J Prosthodont. 1999;12(2)111-121.
43. Levine RA, Shanaman RH. Translating clinical outcomes to patient value: an evidence-based treatment approach. Int J Periodontics Restorative Dent. 1995;15(2): 186-200.
44. Spear FM. It’s all about relationships. Advanced Esthetics and Interdisciplinary Dentistry. 2005;1(4):1.
 Figure 1 The patient on presentation day of traumatic injury to tooth No. 8 to the restorative dentist's office. Note significant diastema at presentation between teeth Nos. 8 and 9.  |  | |
| Figure 2 The fractured coronal portion was removed. | Figure 3 Preoperative PA radiograph of teeth Nos. 7 and 8. | |
 |  | |
| Figure 4 Lingual view of endodontic obturation on tooth No. 8. Note extension of the fracture line subgingivally. | Figure 5 Completion of endodontics with fill of composite resin. Endodontics was then completed for tooth No. 7 (lateral incisor). Note the fracture line to osseous crest for tooth No. 8. An acrylic provisional was placed for tooth No. 8, prepared through the biologic width to gain retention, and cemented with permanent cement. | |
 |  | |
| Figure 6 Presentation to the periodontist's office. After case presentation forced eruption was commenced with acid-etching of teeth Nos. 6, 7, 9, and 10 on the mid-facial enamel portion of the crowns. | Figure 7 Brackets were bonded first on teeth Nos. 6, 7, 9, and 10 for passive bracket engagement with a 0.012 round wire (nickel titanium) followed by apically positioning the bracket for tooth No. 8 approximately 2 mm to allow wire engagement. | |
 |  | |
| Figure 8 Engagement of the wire into tooth No. 8 bracket causes an offset in the wire and its desire to erupt the tooth by its memory to straighten. The temporary crown was reduced 2 mm to 3 mm incisally to allow unimpeded coronal movement of the tooth without interference from the mandibular incisors. | Figure 9 After 2 weeks, the wire is straight and passive; acrylic is placed above the bracket to allow further eruption without replacing it. | |
 |  | |
| Figure 10 Offset of the 0.012 round nickel titanium wire apical to the acrylic allows continued eruption of tooth No. 8. | Figure 11 Tooth No. 8 has erupted approximately an additional 2 mm to 3 mm and is nearly straight. The temporary crown was again reduced incisally and the surgical flap procedure was scheduled 1 week later to anticipate continued eruption of an additional 1 mm. Note the significant eruption of the soft tissue for tooth No. 8. | |
 | Figure 12 Radiograph taken the day of the surgical flap procedure. Note the amount of eruption achieved (approximately 5 mm to 6 mm). Compare with Figure 5. The mesial angular bony discrepancy (termed "lipping") for tooth No. 8 was corrected at the time of surgery. | |
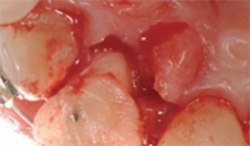 |  | |
| Figure 13 The lingual view at the time of surgical entry to correct soft and hard tissues for tooth No. 8 only. Although the flap extended from the mesial of tooth No. 7 to the mesial of tooth No. 9, the only instrumentation was around tooth No. 8 via ostectomy and gingivectomy. | Figure 14 Facial view of the corrected soft tissue after crown lengthening of tooth No. 8. | |
 |  | |
| Figure 15 Tooth No. 8 was prepared to place a new temporary crown approximately 3 weeks after surgery, with margins placed only to marginal tissues to allow further maturation of the biologic width and sulcular area. | Figure 16 Lingual view of prepared tooth No. 8 with adequate tooth structure now available to place a conventional full-coverage porcelain crown after additional healing of 2 months and completion of orthodontics to move tooth No. 10 into a better arch position for restorative dentistry. Note the facial rotation of this tooth. | |
 |  | |
| Figure 17 With a new second temporary in place for tooth No. 8, the interproximal of both teeth Nos. 8 and 9 were stripped, teeth No. 6 through 8 were common-tied (0.010 dead soft wire) with the goal of dragging tooth No. 9 mesially to provide room for tooth No. 10 to better enter the arch form. A 0.018 round nickel titanium wire was used. | Figure 18 Completion of orthodontic therapy on tooth No. 10 with the creation of adequate space mesially for a proper restorative-sized lateral incisor to be fabricated as a porcelain veneer. | |
 Figure 19 Laboratory casts (lingual view). Porcelain veneers were fabricated for teeth Nos. 6, 7, 9, and 10 and a full-coverage porcelain crown for was fabricated for tooth No. 9. |  | |
| Figure 20 Full facial view of the smile posttreatment. | ||
 |  | |
| Figure 21 Close-up smile view posttreatment. Note that the gingival symmetry was able to be maintained. | Figure 22 Clinical view with lips retracted. Note that gingival health and interproximal papillary locations are very close to pretreatment with gingival health noted around all of the restorations. Compare with Figure 1; this is 2 years posttreatment. | |
 Figure 23 Hawley appliance was fabricated and used as a postorthodontic retainer. |  | |
| Figure 24 Two years after completion of the case. | ||
| About the Authors | ||
 Robert A. Levine, DDS Robert A. Levine, DDSPrivate Practice Pennsylvania Center for Dental Implants & Periodontics Philadelphia, Pennsylvania Clinical Associate Professor in Post-Graduate Periodontics, Implantology, and Perio-Prosthesis School of Dental Medicine University of Pennsylvania Philadelphia, Pennsylvania | ||
 Don G. Katz, DDS, MAGDM Don G. Katz, DDS, MAGDMPrivate Practice Pennsylvania Center for Dental Excellence Philadelphia, Pennsylvania | ||

