
Considerations for Vital Nightguard Tooth Bleaching with 10% Carbamide Peroxide After Nearly 20 Years of Proven Use
Van B. Haywood, DMD
This article offers a reflective look at the considerations for administering 10% carbamide peroxide/nightguard tooth whitening based on what has been learned from ongoing clinical research. Additionally, concerns are raised regarding new approaches to tooth bleaching that may impact the dental profession's credibility and ethical standards toward patient treatment. Subsequent articles in this series by Yiming Li, DDS, MSD, PhD, and Ralph Leonard, DDS, MPH, will discuss in more detail the overall safety afforded by today's whitening alternatives and the efficacy of available bleaching methods, respectively.
Dentists and dental patients continuously seek effective means to simply and conservatively achieve more esthetic smiles. Since it was first described in the literature in 1989,1 vital nightguard tooth whitening using 10% carbamide peroxide has become an integral part of routine dental care for appropriately identified patients of various ages who present with different types of tooth discolorations.
The basic formulation of 10% carbamide peroxide solution is equivalent to a 3.5% hydrogen peroxide solution. Carbamide peroxide is basically hydrogen peroxide in urea. Urea contributes to the whitening solution’s slow release: 50% of its active agents in the first 2 to 4 hours, then the remaining 50% in up to 10 hours. Hydrogen peroxide whitening materials will release 50% of their active agents in 30 minutes with the remainder gone within an hour. Therefore, carbamide peroxide whiteners are intended to be worn for extended periods because their effectiveness is achieved slowly, but more efficiently, per application.
This author advocates a nonscalloped, no-reservoir, horseshoe-shaped soft tray (Figure 1A and Figure 1B). However, a different tray design may be required for patients with special considerations, such as those with temporomandibular joint disorder2 (for whom the tray design should not change occlusion) or those who need to bleach only a single dark tooth (Figure 2).3
EFFICACY
When the concept of nightguard vital tooth bleaching was first introduced, the mechanism by which the teeth were whitened was thought to be the removal of extrinsic stains. However, researchers noted that the actual intrinsic color of the teeth was changed,4,5 even if the color was genetically determined, because the effects of the whitening agent extended to portions of the tooth not in direct contact with the solution. For example, a person born with yellow teeth could undergo vital nightguard tooth whitening and achieve “normally” white teeth (Figure 3A and Figure 3B).
Because the tooth is a semipermeable membrane, substances such as peroxide, water, and urea pass freely through the enamel and dentin to the pulp within 5 minutes to 15 minutes. Once the bleaching agent reaches the dentin (from which teeth get their intrinsic color) color change occurs.5 Of note is the fact that the color change occurs uniformly from the dentin nearest the dentin-enamel junction to the dentin nearest the pulp.4,5
Vital nightguard tooth whitening has been shown to be effective for conservatively enhancing the smiles of children whose primary teeth have been discolored as a result of trauma6 as well as those of adults with intrinsic stains from tetracycline treatments (Figure 4A and Figure 4B). Treatment of tetracycline stains requires an average bleaching time of between 2 months to 6 months.7,8 Additionally, 10% carbamide peroxide and a custom-fitted soft tray for nighttime use have demonstrated long-term efficacy for the removal of brown stains9 in addition to stains from fluorosis (eg, brown or white). In both instances, bleaching is performed nightly for up to 6 weeks. Teeth with severe nicotine staining also have been successfully whitened through this process when the regimen is followed for between 1 month and 3 months.
The color of teeth does get progressively whiter as the bleaching regimen continues. However, teeth do reach a maximum lightness and, regardless of what agents are subsequently used, no further lightening will occur. When the whitening process is complete, the whitened shade of the teeth will slightly darken by approximately half a shade, which is where the teeth will likely stay for years. For this reason, final shades should not be determined immediately postbleaching.10
Although using a stronger concentration of whitening agent will whiten teeth somewhat faster,11 teeth can only change color at a certain rate. A quicker two-tab color change has been noted for 10% and 16% carbamide peroxide compared to 5% carbamide peroxide at days 8 and 15. However, continuation of the 5% treatment to 3 weeks resulted in shades that approached the 2-week 10% and 16% values.11
Teeth also seem to have a “maximum whiteness” they can obtain from bleaching. Once the color has reached this point, additional treatment does not increase whiteness. There is no reliable method to predict how white a patient’s teeth are able to become, and the treatment time can vary from 3 days to 6 weeks to achieve that level of whitening. Ideally, the patient should continue whitening until either he or she is satisfied with the color change or there is no additional color change over a 7-day period (or a month for tetracycline-stained teeth).12
A caveat of tooth bleaching is that the roots of teeth do not change color, regardless of the technique used. The dentin in tooth roots is significantly different from the dentin under the enamel (ie, different tubular shapes and densities). Therefore, exposed and discolored roots will not drastically change color. Instead, composite restorations may need to be placed if the patient desires a uniform appearance of all visible tooth structure postbleaching.
SAFETY
When properly supervised and dentist-monitored, vital nightguard tooth whitening with 10% carbamide peroxide is safe and effective, with no long-term posttreatment side effects (eg, no external cervical resorption, gingival index and tooth vitality findings within normal range, no restorations or root canal therapy required as a result of whitening) reported at approximately 10 years posttreatment.8,13 At 10 years postbleaching, scanning electron microscopic observations have not shown substantial differences between treated and untreated tooth surfaces, and 43% of bleaching patients at recall said that color stability may last approximately 10 years.13 Other research suggests that this type of tooth whitening also does not produce any detrimental effects on soft tissues.14
Although there may be concerns regarding the effect of the whitening agent on enamel, research indicates that the amount of calcium lost from exposure to carbamide peroxide is the equivalent of that lost when teeth are exposed to a cola beverage for 2.5 minutes (the amount of time necessary to drink a 16-oz beverage).15 In fact, the researchers concluded that the amount of calcium loss was small and may not be clinically significant.15
The typical result of nightguard bleaching is a whiter and more “normal” appearance of the teeth—lighter at the incisal edge and slightly darker at the gingival margin (Figure 5A and Figure 5B). One of the benefits of tooth whitening is that it reduces the aged look patients may have as a result of the appearance of their teeth. Other benefits include an enhanced self-image, a new dedication toward oral hygiene, and a heightened awareness of other problems with their dentition (eg, occlusion, alignment, gingival contours, etc) that may motivate patients to undergo additional necessary treatment.
THE FIRST CONSIDERATION
When cost, safety, and effectiveness of vital nightguard tooth bleaching are considered collectively, nightguard vital bleaching with 10% carbamide peroxide in a custom-fitted tray for changing the appearance of teeth should remain the first consideration for conservatively enhancing smile esthetics. Although bleaching may not be effective in all cases, vital nightguard tooth whitening with 10% carbamide peroxide does not compromise or eliminate any future treatment options.3 Rather, it may precede other treatments that may be necessary to achieve the patient’s desired results, including macroabrasion and direct composite bonding, esthetic contouring, or more invasive indirect restorative techniques (eg, veneers or crowns).
DIAGNOSING DISCOLORATION AND MANAGING PATIENT EXPECTATIONS
Once a patient has expressed a desire to undergo tooth whitening—either as a result of questions by the clinician (eg, “Before I place these composites or prescribe this crown, have you ever thought of whitening your teeth? Now would be the time to do so.”) or curiosity about an in-office poster or presentation—the cause of the patient’s tooth discoloration must be diagnosed. Only then can the appropriate treatment be administered. Tooth discoloration could result from trauma, genetics, extrinsic stains, medications, ingested foods/minerals, decay, or lack of vitality. Therefore, changing the color of a patient’s teeth could involve vital nightguard tooth whitening or perhaps the placement of composite restorations or endodontic therapy.
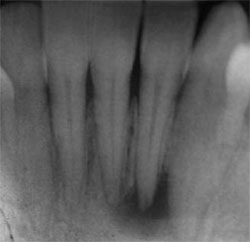
Because internal resorption could contribute to tooth discoloration, it is important to obtain a baseline radiograph of all potential tooth-whitening patients. Although the clinical examination may not reveal anything unusual, the radiograph may uncover abscesses, previous root canals, lesions, and/or other underlying causes for the tooth discoloration (Figure 6A; Figure 6B; Figure 6C).
During the examination it is also important to perform a smile analysis to determine if further treatment may be required, such as replacing existing restorations. In particular, patients must be counseled that existing restorations may no longer blend with their smile once their teeth are bleached. They must also understand the potential outcome of whitening (eg, some provisional restorative materials could exhibit an orange discoloration16), that the restorations will need to be replaced if they want them to match their natural tooth color, and that they will need to be financially prepared for any new restorations.
Patients should be informed that tooth whitening will not correct every defect, and dentists must provide complete disclosure to the patient of his or her condition (eg, occlusal problems, orthodontic problems, caries, or existing restorations). Patients whose teeth are too translucent should know in advance that they may not achieve the whitening results they are hoping for. In that case, an alternative or additional treatment (eg, composites or veneers) should be considered. Patients with amalgam fillings in esthetic areas (the tooth structure around certain older brands of amalgam has been shown to turn green after whitening for long periods of time) may need to have those restorations replaced with composites before bleaching.17 However, generally speaking, composite or other restorations are replaced at least 2 weeks after bleaching to allow for color stabilization and sufficient bond strengths.18,19
Depending on the type of preexisting restorations and the dentistry that has been previously performed, the dentist may need to strongly advise the patient against whitening. For example, if a patient who desires bleaching presents with a crown restoration on a tooth that has undergone a root canal and apicoectomy, which would need to be replaced postbleaching to match the new tooth shade, bleaching may be contraindicated because of the risk of ultimately losing the tooth.
Conversely, if a patient is dissatisfied with the appearance of preexisting porcelain veneer restorations, dentists can recommend 10% carbamide peroxide nightguard bleaching. Using a custom-fitted tray with no reservoirs and no gingival scalloping, the color of the tooth structure under the veneers can be whitened from the lingual aspect and, hence, the appearance of the veneers can be changed.20 Additionally, tooth staining around veneer restorations can be removed with nightguard bleaching, after which the veneers can be resealed with a dentin bonding agent.
Patient expectations should be managed in terms of what bleaching results are possible and how long the process could take. Nighttime wear of the custom-fitted soft tray is still preferred. Accordingly, most bleaching regimens with 10% carbamide peroxide require 2 weeks to 6 weeks to achieve the patient’s desired results.
Other indications may take longer and/ or require additional efforts, such as macroabrasion in the cases of endemic dental fluorosis21 and stark white spots that will not “disappear” into the tooth even after bleaching. Nightguard vital bleaching should be performed first followed by the macroabrasion. For example, if the white areas of the tooth are sanded down to the dentin, and it is found that the discoloration is worsening as the sanding goes deeper, then a composite restoration would be required before bleaching. Macroabrasion can be completed using various pairings of diamond and carbide burs, abrasive discs, rotary polishing points, and diamond polishing pastes.21
RELIEVING SENSITIVITY WITH POTASSIUM NITRATE
In the attempt to achieve faster whitening results, some clinicians use higher concentrations of whitening agents, which contribute to greater sensitivity. Most sensitivity occurs within the first 2 weeks of bleaching, regardless of the total length of treatment. However, no statistical relationship has been shown to exist between age, gender, allergy, tooth characteristics (ie, gingival recession, defective restorations, abfraction lesions, enamel-cementum abrasion), or the dental arch bleached and the development of side effects from vital nightguard tooth bleaching.22 However, researchers found that patients who change the whitening solution more than once a day reported statistically significantly more side effects than those who did not change the whitening solution during their usage time.22
The traditional treatment for sensitivity has been fluoride, which is a tubular blocker. However, 3% to 5% potassium nitrate, which penetrates the enamel and dentin and reaches the pulp to produce a numbing effect, in a tray for 10 minutes to 30 minutes before bleaching is also effective in reducing sensitivity.23 Five percent potassium nitrate is currently available in over-the-counter (OTC) desensitizing toothpastes24 as well as some professionally-dispensed products.
When instructing patients to use desensitizing toothpaste in their tray before bleaching to relieve sensitivity, be sure to advise them to use brands that do not contain sodium laurel sulfate, which causes gingival irritation. Additionally, the use of a potassium nitrate plus fluoride dentifrice for 2 weeks before bleaching (as well as throughout the process) has been suggested as a useful adjunct for the management of sensitivity caused by professionally dispensed bleaching products.24
To further help in relieving sensitivity, some manufacturers have added potassium nitrate to their whitening solutions. It has been shown that a 10% carbamide peroxide bleaching gel containing potassium nitrate and fluoride produces less tooth sensitivity than the control bleaching gel during a 2-week at-home bleaching treatment.25
WHITENING ALTERNATIVES
From in-office bleaching to dentist-monitored at-home treatments and abrasive dentifrices that remove extrinsic stains to other OTC products, the dental profession is brimming with purportedly effective methods for whitening and brightening smiles. Current research, however, suggests that one in-office whitening appointment is insufficient to achieve the results that can be obtained from take-home nighttime tray bleaching.26 Additionally, the majority of published articles regarding in-office whitening lights indicate that the use of light does not demonstrate any benefit over chemically activated tooth whitening.27
Some OTC tooth-whitening products, such as disposable strips with various concentrations of hydrogen peroxide, have been shown to be effective in whitening teeth and changing intrinsic tooth color.28,29 However, clinicians still are challenged to educate patients about other OTC tooth-whitening alternatives, including those sold exclusively on television and/or which claim to be the same as what is available at a dentist’s office (eg, a tooth-whitening light for home use). Potential adverse effects may occur from inappropriate applications, abuses, or the use of inappropriate products.30 The tooth whitening experience is best maximized through the use of dentist-monitored at-home whitening systems.30
CONCLUSION
Whitening is best performed in a professionally supervised manner following a thorough examination and proper diagnosis. It is this author’s opinion after reviewing the current research that 10% carbamide peroxide in a custom-fitted soft tray is the most ideal whitening treatment. However, other treatments may be indicated based on patient preference, lifestyle, finances, and limitations to whitening effectiveness (eg, tetracycline stains, very stark white spots, extensive restorations, or exposed root surfaces).
First and foremost, dentists have an obligation to care for their patients by providing the best treatment for them. Therefore, it is incumbent upon dentists who provide vital tooth whitening services to inform patients of the benefits and risks of different options within this category, additional treatments that may be required (eg, replacing existing restorations), and a cost/benefit analysis of all potential treatment options. Additionally, the recommendations provided should be based on as much scientific evidence as possible.
References
1. Haywood VB, Heymann HO. Nightguard vital bleaching. Quintessence Int. 1989;20(3): 173-176.2. Robinson FG, Haywood VB. Bleaching and temporomandibular disorder using a half tray design: a clinical report. J Prosthet Dent. 2000;83(5): 501-503.
3. Caughman WF, Frazier KB, Haywood VB. Carbamide peroxide whitening of nonvital single discolored teeth: case reports. Quintessence Int. 1999;30(3): 155-161.
4. Haywood VB, Leech T. Heymann HO, et al. Nightguard vital bleaching: effects on enamel surface texture and diffusion. Quintessence Int. 1990;21(10):801-804.
5. McCaslin AJ, Haywood VB, Potter BJ, et al. Assessing dentin color changes from nightguard vital bleaching. J Am Dent Assoc. 1999;130(10):1485-1490.
6. Brantley DH, Barnes KP, Haywood VB. Bleaching primary teeth with 10% carbamide peroxide. Pediatr Dent. 2001;23(6):514-516.
7. Leonard RH Jr, Haywood VB, Eagle JC, et al. Nightguard vital bleaching of tetracycline-stained teeth: 54 months post treatment. J Esthet Dent. 1999;11(5): 265-277.
8. Leonard RH Jr, Haywood VB, Caplan CJ, et al. Nightguard vital bleaching of tetracycline-stained teeth: 90 months post treatment. J Esthet Restor Dent. 2003;15(3):142-152.
9. Haywood VB, Leonard RH. Nightguard vital bleaching removes brown discoloration for 7 years: a case report. Quintessence Int. 1998;29(7):450-451.
10. Matis BA. Tray whitening: what the evidence shows. Compend Contin Educ Dent. 2003; 24(4A):354-362.
11. Leonard RH, Sharma A, Haywood VB. Use of different concentrations of carbamide peroxide for bleaching teeth: an in vitro study. Quintessence Int. 1998;29(8):503-507.
12. Haywood VB. Treating sensitivity during tooth whitening. Compend Contin Educ Dent. 2006;26(9):11-20.
13. Ritter AV, Leonard RH Jr, St Georges AJ, et al. Safety and stability of nightguard vital bleaching: 9 to 12 years post-treatment. J Esthet Restor Dent. 2002;14(5):275-285.
14. Curtis JW, Dickinson GL, Downey MC, et al. Assessing the effects of 10 percent carbamide peroxide on oral soft tissues. J Am Dent Assoc. 1996;127(8): 1218-1223.
15. McCracken MS, Haywood VB. Demineralization effects of 10 percent carbamide peroxide. J Dent. 1996;24(6):395-398.
16. Robinson FG, Haywood VB, Myers M. Effect of 10 percent carbamide peroxide on color of provisional restoration materials. J Am Dent Assoc. 1997;128(6):727-731.
17. Haywood VB. Greening of the tooth-amalgam interface during extended 10% carbamide peroxide bleaching of tetracycline stained teeth: a case report. J Esthet Restor Dent. 2002;14(1):12-17.
18. Cavalli V, Reis AF, Giannini M, et al. The effect of elapsed time following bleaching on enamel bond strength of resin composite. Oper Dent. 2001;26(6):597-602.
19. Lai SC, Tay FR, Cheung GS, et al. Reversal of compromised bonding in bleached enamel. J Dent Res. 2002;81(7):477-481.
20. Haywood VB, Parker MH. Nightguard vital bleaching beneath existing porcelain veneers: a case report. Quintessence Int. 1999;30(11): 743-747.
21. Bodden MK, Haywood VB. Treatment of endemic fluorosis and tetracycline staining with macroabrasion and nightguard vital bleaching: a case report. Quintessence Int. 2003;34(2):87-91.
22. Leonard RH Jr, Haywood VB, Phillips C. Risk factors for developing tooth sensitivity and gingival irritation associated with nightguard vital bleaching. Quintessence Int. 1997;28(8):527-534.
23. Haywood VB, Caughman WF, Frazier KB, et al. Tray delivery of potassium nitrate-fluoride to reduce bleaching sensitivity. Quintessence Int. 2001;32(2):105-109.
24. Haywood VB, Cordero R, Wright K, et al. Brushing with a potassium nitrate dentifrice to reduce bleaching sensitivity. J Clin Dent. 2005;16(1):17-22.
25. Tam L. Effect of potassium nitrate and fluoride on carbamide peroxide bleaching. Quintessence Int. 2001;32(10):766-770.
26. de Silva Gottardi M, Brackett MG, Haywood VB. Number of in-office light-activated bleaching treatments needed to achieve patient satisfaction. Quintessence Int. 2006;37(2):115-120.
27. Kugel G, Papathanasiou A, Williams AJ 3rd, et al. Clinical evaluation of chemical and light-activated tooth whitening systems. Compend Contin Educ Dent. 2006;27(1):54-62.
28. Shahidi H. Barker ML, Sagel PA, et al. Randomized controlled trial of 10% hydrogen peroxide whitening strips. J Clin Dent. 2005;16(3): 91-95.
29. Cooper JS, Bokmeyer TJ, Bowles WH. Penetration of the pulp chamber by carbamide peroxide bleaching agents. J Endod. 1992;18(7):315-317.
30. Li Y. The safety of peroxide-containing at-home tooth whiteners. Compend Contin Educ Dent. 2003;24(4A):384-389.
 |  | |
| Figure 1A View of a nonscalloped, noreservoir upper arch tray in the mouth. | Figure 1B View of the same tray design for the lower arch on a model. | |
 | ||
| Figure 2 Tray design used when whitening a single dark tooth without altering the color of the adjacent teeth. | ||
 |  | |
| Figure 3A Preoperative view of a patient with genetically yellow teeth. | Figure 3B View of the same patient after tooth bleaching. | |
 |  | |
| Figure 4A Initial view of an adult patient with severe tetracycline stains. | Figure 4B Postbleaching view of the smile after a regimen of nighttime vital tooth bleaching with 10% carbamide peroxide. | |
 |  | |
| Figure 5A Prebleaching view of an average patient's teeth. | Figure 5B Postbleaching view of the same patient. Note the enhanced esthetics and uniform color change. | |
 | ||
| Figure 6A Preoperative image of a patient presenting with a discolored tooth. The patient experienced no pain or discomfort in this tooth. | ||
 | 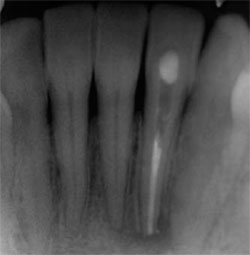 | |
| Figure 6B View of the baseline radiograph, which shows the underlying cause of the tooth discoloration: an abscess. | Figure 6C Postendodontic treatment view of the patient. The patient is now ready for bleaching treatment. | |
| About the Author | ||
 Van B. Haywood, DMD Van B. Haywood, DMD Department of Oral Rehabilitation Medical College of Georgia School of Dentistry Augusta, Georgia | ||

