
Intraoral Porcelain Repair
Lorin Berland, DDS
Improvements in all-ceramic technology have heralded a revolution in esthetic dentistry. It has been estimated that there were approximately54 million all-porcelain restorations placed in the United States last year alone. However, porcelain is brittle. Even under ideal circumstances, long-term functioning in the oral environment can eventually lead to porcelain fractures. Unfortunately, as more porcelain goes in the mouth, it is inevitable that more porcelain will fracture. Conventional wisdom requires a fractured porcelain restoration to be completely removed and replaced. This requires anesthetic, rotary instruments, impressions, temporization, and a second appointment for cementation. These are some of the drawbacks in esthetic dentistry, which can be very frustrating for both the patient and the dentist (especially in the case of an anterior tooth).
A great improvement would be if porcelain could be immediately and predictably repaired chairside with composite resin. In the past, the problem was how to provide an adequate adhesive bond between the existing porcelain and the new composite.1 Adhesion between porcelain and composite can be accomplished in a combination of 3 ways:
- Macromechanically (ie, sandblasting with 5-mm aluminum oxide).2
- Micromechanically (ie, acid etching the porcelain with 6% hydrofluoric acid).3
- Chemical retention (applying coupling agents and resins).4
Recently, there has been a greater understanding and improvement in the science of adhesion dentistry. This area is of particular importance to the bonding of composite resin material to various substrates, especially porcelain.5 There are currently a variety of porcelain repair kits available,6 which usually consist of a porcelain etch and a silane primer.7 However, all of these kits have a simple problem. Silane is extremely reactive and volatile, and it begins to lose its viability as soon as the bottle is opened. Further, most of the silane is packaged in plastic, which means the silane is constantly exposed to light and air from the date it was packaged. This is certainly not the ideal method for storing these chemicals.8 A new system, Versa-Link® (Sultan Healthcare, Inc, Englewood, NJ), takes a different approach. The silane porcelain primer is delivered in hermetically sealed amber glass ampules. This 1-dose delivery system keeps the primer pure and stable for up to 2 years. Chemically and clinically, this translates to a better porcelain bonding system (Figure 1).
Clinical Case
The patient presented with 6 porcelain veneers, which were placed 13 years ago. After an accident, the gingival third of the veneer on the lateral incisor fractured (Figure 2). This created an immediate dilemma for the patient. She was in the public eye, traveled extensively on business, and did not have time for multiple extended appointments. We presented the patient with 2 options:
- The first option was to remove the veneer and replace it. This would require anesthesia, drilling, an impression, a temporary, and another appointment to cement the new veneer. In the meantime, a temporary would be placed, which would hopefully stay in place until placement of the final veneer (Figure 3).
- The second option was to repair the veneer intraorally using Versa-Link. The restoration would be completed immediately, no anesthesia would be required, and there would be little guesswork. An additional benefit of using this option was that if it did not work, option 1 could still be considered.
The second option was chosen. After polishing, the appropriate shade of composite was chosen. A mock-up of the resin allowed us to predict an acceptable match. The tooth was isolated with Dead Soft Metal Matrix Strips (DenMat, Santa Maria, CA). The gingiva and tooth can be protected with Expasyl™ (Kerr Corp., Orange, CA) or a liquid rubber dam. In this case, Expasyl was used to dry and protect the tissue, and a cured liquid rubber dam was used on the exposed tooth. With protection in place, the fractured porcelain was air abraded to increase macro-mechanical retention (Figure 4).
The aluminum oxide was thoroughly rinsed off. With the liquid rubber dam and Expasyl still in place, the 6% hydrofluoric acid porcelain etch was applied to the porcelain (Figure 5). After 90 seconds, the porcelain etch was vigorously washed off using a simultaneous mixture of water and air directed toward the porcelain in an incisal direction, away from the tooth and gum. The liquid dam was removed and the exposed tooth structure was etched with 35% phosphoric etchant for 15 seconds before completely rinsing and drying (Figure 6). The amber glass ampule of Versa-Link silane porcelain primer was opened. A fresh, 1-time application was brushed on the fractured porcelain margins for a minimum of 3 to 4 minutes (Figure 7) and air dried. The porcelain repair was then completed using bonding agents and composite resin (Figure 8). The restoration was polished using first Topex® Brilliance polishing paste (Sultan Healthcare) followed by Topex® Brilliance micrograin paste (Sultan Healthcare) to finish (Figure 9). The patient left smiling (Figure 10).
CONCLUSION
The increased use of all-porcelain restorations will increase the need for intraoral repairs of fractured porcelain. It has been the author’s experience that Versa-Link’s unique packaging increases the clinical longevity of these restorations, resulting in happier patients and happier dentists.
DISCLOSURE
The author receives financial or material support from Sultan Healthcare, Inc.
References
1. Zhukovsky L, Godder B, Settembrini L, et al. Repairing porcelain restorations intraorally: techniques and material. Compend Contin Educ Dent. 1996;17(1): 18-30.2. Chung KH, Hwang JC. Bonding strengths of porcelain repair systems with various surface treatments. J Prosthet Dent. 1997;78(3): 267-274.
3. Goia T, Leite F, Bottino M, et al. Effect of various chairside surface-conditioning methods for ceramic repair. Presented at:IADR/AADR/CADR 83rd General Session; Mar 9-12, 2005; Baltimore, MD.
4. Hooshmand T, van Noort R, Keshvad A. Bond durability of the resin-bonded and silane treated ceramic surface. Dent Mater. 2002;(10):179-188.
5. Della Bona A, Shen C, Anusavice KJ. Work of adhesion of resin on treated lithia disilicate-based ceramic. Dent Mater. 2004;20(4): 338-344.
6. Haselton DR, Diaz-Arnold AM, Dunne JT Jr. Shear bond strengths of 2 intraoral porcelain repair systems to porcelain to metal substrates. J Prosthet Dent. 2001;86(5):526-531.
7. Kupiec KA, Wuertz KM, Barkmeier WW, et al. Evaluation of porcelain surface treatments and agents for composite-to-porcelain repair. J Prosthet Dent. 1996;76(2):119-124.
8. Llobell A, Nicholl JL, Kois JC, et al. Fatigue life of porcelain repair systems. Int J Prosthodont. 1992;5(3): 205-213.
 |  | |
| Figure 1 The Versa-Link® Kit. | Figure 2 The fractured veneer. | |
 |  | |
| Figure 3 The composite shade being matched. | Figure 4 The tooth was isolated and air abraded. | |
 |  | |
| Figure 5 The porcelain was etched with Versa-Link® 6% hydrofluoric acid. | Figure 6 The tooth was etched. | |
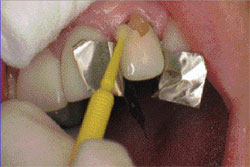 |  | |
| Figure 7 The Versa-Link® silane porcelain primer. | Figure 8 The composite resin was applied. | |
 |  | |
| Figure 9 Topex® Brilliance polishing paste. | Figure 10 The final intraoral porcelain repair. | |
| About the Author | ||
 Lorin Berland, DDS Lorin Berland, DDSPrivate Practice Dallas, Texas | ||

