
Activ GP™: A Single-Cone Obturation Technique
Kenneth Koch, DMD; Dennis G. Brave, DDS
Endodontics has been witness to many obturation techniques, and there are clinicians who can obtain excellent results with any of these methods. However, there are 2 goals of obturation that have not been addressed with these methods. The first is to create a hermetic seal within the root canal system. The second is to establish a technique that gives the greatest majority of clinicians the ability to produce superior results. It is with these goals in mind that the Activ GP™ Obturation System was developed. This technique uses improved glass ionomer technology and combines it with advanced material science to result in a technique that provides both hermetic seal and superior results.
In the pursuit of a true single-cone technique, glass ionomer is attractive because of its superior biocompatibility and physical properties. The merits of glass ionomer are numerous. First, in addition to having the capability of wet bonding (ie, it does well in a moist environment), glass ionomer actually creates an ionic bond to the dentin. This bond is critical in terms of a monobloc (hermetic seal). Secondly, glass ionomers are nonresorbable, which is critical in a single-cone or sealer-based obturation technique. Because of the great biocompatibility of glass ionomer, the fact that it does not undergo resorption is not a problem. In fact, glass ionomer cements have been used routinely in orthopedic surgery to hold fixtures or fragments in place. Furthermore, the setting time of glass ionomer is such that the clinician can prepare a post and place it at the same appointment as the endodontic procedure.
Monobloc: Challenges
Although the merits and properties of glass ionomer were well known, there remained some limitations with the first-generation glass ionomer sealers. The handling characteristics of these sealers were a challenge and they generally did not produce a sufficient working time. Furthermore, they did not demonstrate a bond to gutta percha. Consequently, altering the properties of glass ionomer sealer to meet the requirements of a monobloc was the first challenge.
The first change made was with the working time. By modifying the particle sizes of the glass ionomer, the working time has been extended. The working time of Activ GP sealer is 12 minutes on a paper pad and 20 minutes on a chilled glass slab. Furthermore, Activ GP sealer comes in a powder/liquid combination that allows the assistant to mix it to a consistency that is favorable for the clinician and the individual case.
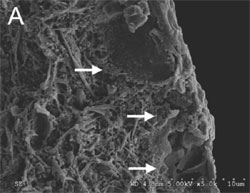
Although changes were made with the sealer, the lack of a bond between the sealer and the gutta percha still remained a challenge. This challenge was met by taking silanated glass ionomer particles (present in the sealer) and placing them into the gutta percha cones at a percentage that does not affect the properties of gutta percha. Additionally, the impregnated cones were coated with glass ionomer particles at a thickness of 2 µm. Scanning electron microscopy shows that there is no gap between the coating of glass ionomer and the glass ionomer-impregnated gutta percha cones (Figures 1A and 1B).
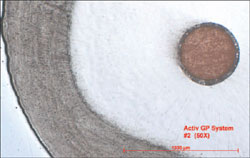
As a result of these enhancements, Activ GP sealer now has the ability to bond directly to the Activ GP points. The result is a monobloc between the canal wall, the Activ GP sealer, and the master cone. This allows the creation of a true hermetic seal, which is a very significant development in endodontics (Figures 2 and 3).
Activ GP System
The Activ GP System (Figure 4) is ISO sized and colored and is available in two types: a traditional design and an enhanced version (Activ GP Plus). Activ GP Plus uses calibration rings for easy depth measurement and a unique barrel handle which, when placed with an insertion instrument (transporter), facilitates easy placement into the canal (Figures 5A and 5B -).
This Activ GP Obturation System delivers a true monobloc obturation result through a single-cone technique. However, the system still remains precision-based, which means it requires synchronicity between the file and the master cone. The sizes of Activ GP points are consistently accurate and are verified as such by laser measurement. In fact, all Activ GP points are laser verified to match the preparations made by the .04 or .06 tapered EndoSequence file system. The precision matching of the primary cone to the preparation is very important with a single-cone technique because the accuracy of the cones to the preparation minimizes the amount of sealer and any potential shrinkage.
Technique
The technique associated with Activ GP is straightforward. After completion of a constant taper preparation and verification by radiograph of the fit of the Activ GP cone, a hand file is chosen that matches the final size of the preparation. The file is coated with the Activ GP sealer and taken to working length. It is recommended that this process is repeated a second time.
After placement of the sealer, the Activ GP cone is coated with sealer and slowly inserted into the canal to its working length. As a result of the endodontic synchronicity between the file and master cone, hydraulics is generated, which moves the sealer into lateral canals. However, because it is inserted slowly, any excess sealer will extrude out coronally alongside the cone (Figure 6).
After the cone has been inserted to working length and verified with a digital image or radiograph, it is recommended that the cone be seared off at the orifice and that an additional 1 mm to 2 mm of gutta percha be removed from the canal. After removal of the gutta percha, the Activ GP sealer is placed on top of the cone to act as a final canal cap. This procedure will effectively prevent coronal leakage, which can contaminate the completed root canal.
Conclusion
The Activ GP obturation technique meets two significant criteria. First is the introduction of improved glass ionomer technology that can result in a true monobloc obturation, which allows the creation of a hermetic seal within the root canal. Second, a simple, sophisticated technique has been introduced, which gives the greatest majority of practitioners the ability to produce superior obturation results. The patient is the true beneficiary of this technology (Figures 7, 8, 9).
For More Information
Brasseler USA
Phone: 1-800-841-4522
E-mail: info@brasselerusa.com
Web: Brasselerusa.com
 |
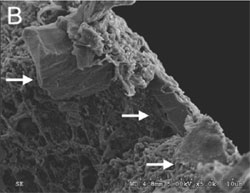 |
| Figures 1A and 1B Cross sections of the coated gutta percha points. The arrows indicate the coating on the gutta percha point. The thickness of the coating is 2 µm. On close inspection, no interface is observed between the surface of the gutta percha point and the glass ionomer coating because of the excellent adhesion (SEM by Quanzu Yang). | |
 |
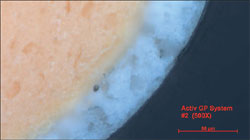 |
| Figure 2 Light refractive metallograph demonstrating the relationship between the cementum, dentin, Activ GP sealer, and the master cone. The consistency of the preparation (EndoSequence), along with the monobloc obturation achieved with the Active GP System demonstrates endodontic synchronicity. | Figure 3 Very high magnification image of the bond created with Activ GP. Note the glass ionomer particles in the gutta percha. |
 |
 |
| Figure 4 The Activ GP Precision Obturation System. | Figures 5A and 5B Activ GP Plus cones come with length markings to ensure precision of insertion into the respective root canals. |
 |
 |
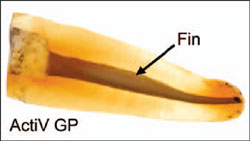
| Figure 6 Leakage study validating the use of the Activ GP System. Evidence is seen of the Activ GP sealer going entirely into the fins of this tooth. No discernible leakage is seen alongside the sealer. Also, there is no leakage underneath the glass ionomer “canal cap” that was placed on top of the obturated canal. The tooth was fully immersed in India ink for ten days (Leakage study by Koch and Brave). | Figure 7 Clinical case showing lateral canals filled with Activ GP sealer. |
 |
 |
| Figure 8 Clinical case showing premolar and molar obturated with the Activ GP system. | Figure 9 Maxillary molar case. |

